Article Text

Statistics from Altmetric.com
Description
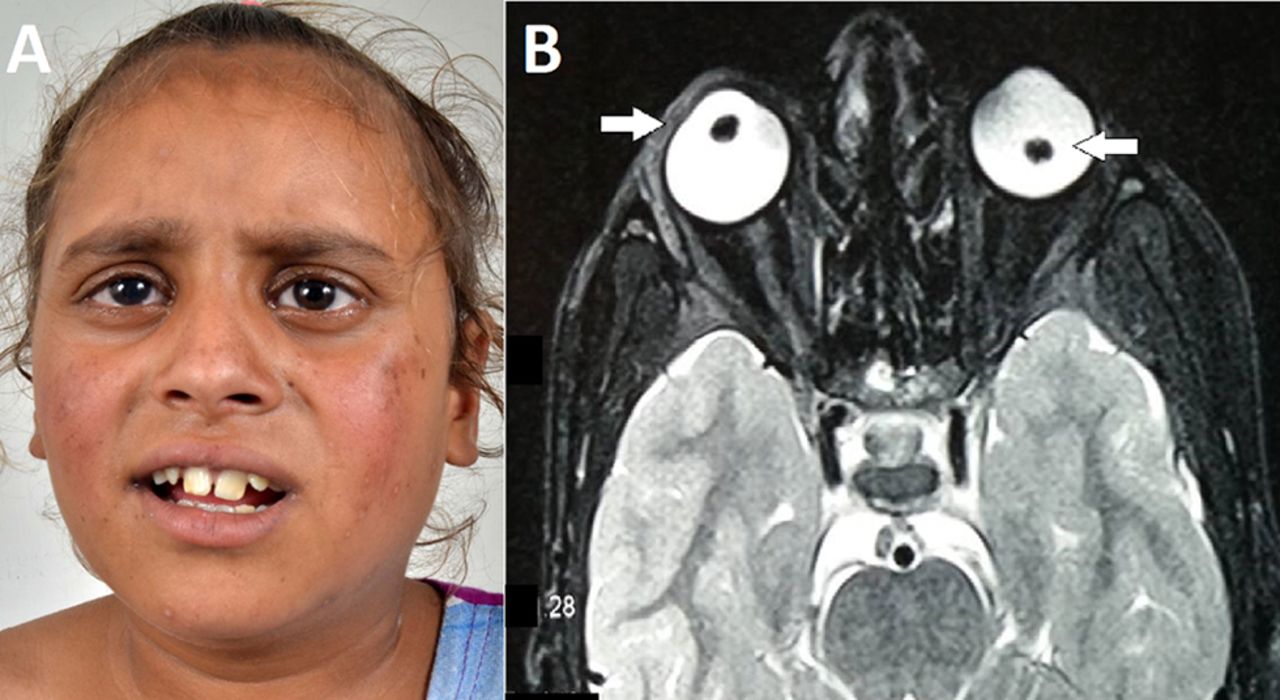
An 8-year-old girl with intellectual disability and severe myopia presented with subacute bilateral painless loss of vision. Anthropometric examination showed a weight of 26 kg (−0.1 Z score), height of 122.5 cm (between −1 and −2 Z score), arm span of 129 cm (6.5 cm longer than the height) and head circumference of 51 cm (between −1 and −2 Z score). Physical examination showed thin, hypopigmented hair with malar rash (figure 1A), acral hyperpigmentation, bilateral inferonasal subluxation of lens and bilateral optic atrophy. Other marfanoid features such as arachnodactyly, high-arched palate, joint hyperlaxity and cardiac anomalies were absent. A clinical diagnosis of classical homocystinuria was considered. Investigations showed elevated plasma homocysteine of 209 µmol/L (range 5–15 µmol/L), urine homocystine of 76 mmol/mol creatinine (range 0–4 mmol/mol creatinine), serum vitamin B12 of 445 pg/mL (211–911 pg/mL), normal methionine of 51 µmol/L (0–75 µmol/L) and a normal carnitine profile, which confirmed our clinical diagnosis. MRI of the brain showed normal parenchyma with bilateral dislocation of lens (figure 1B). She was started on oral pyridoxine, folate and betaine. Currently, after 3 months of treatment, there is improvement in vision and cognitive functions. However, the malar rash is still persistent with only mild reduction in erythema.
{kind=link}
(A) Facial picture of the index patient showing bilateral malar flush noticed since the age of 5 years and thin, hypopigmented and lustreless hair. (B) MRI of brain showing bilateral lens dislocation in the eyes. The rest of the brain parenchyma (not shown) was normal.
Characteristic features of classic homocystinuria caused by cystathionine-beta-synthase deficiency includes developmental delay or intellectual disability, myopia commonly evident after 1 year of age and ectopia lentis usually by 8 years of age, excessive height and limb length, skeletal abnormalities and vascular thromboembolism.1 Less commonly, a peculiar ‘malar’ rash on the cheeks (malar flush) may be seen and may lead to an incorrect diagnosis of systemic lupus in adolescent girls. It can be easily seen after vigorous exercise or after exposure to the cold. The probable biochemical mechanism is inhibition of tyrosinase enzyme by interaction of homocysteine with copper at the active site of tyrosinase,2 and this leads to reduced melanin and manifests as malar rash and fragile hair. Hence, malar flush in a child with lens dislocation and intellectual impairment should lead to a suspicion of classical homocystinuria.
Learning points
Malar rash is an unusual cutaneous manifestation of classic homocystinuria.
Probable mechanism would be attributed to inhibition of tyrosinase enzyme by interaction of homocysteine with copper at active site of tyrosinase.
Malar rash with intellectual disability and lens dislocation would point towards a clinical diagnosis of homocystinuria.
Footnotes
Contributors AGS: Patient management, draft of manuscript and review of literature.
HP: Patient management and review of manuscript.
SA: Analysis and interpretation of biochemical data and manuscript editing.
PS: Clinician-in-charge and critical review of manuscript for intellectual content and final approval of the version to be published.
Competing interests None declared.
Patient consent Consent obtained from guardian.
Provenance and peer review Not commissioned; externally peer reviewed.