Article Text

Statistics from Altmetric.com
Description
A 53-year-old man presented with right-sided sciatic-like pain. He was otherwise asymptomatic with no weakness, sphincter disturbances or gait problems. On examination, upper motor neuron signs were elicited in both lower limbs and an MRI of the whole spine was requested.
MRI showed dorsal tethering of the spinal cord secondary to a fibrous band, associated with two midline lipomas (figure 1). The affected cord segment was triangular in cross section (figure 2), and a syrinx was also observed at the affected level. Radiological appearances were compatible with meningocele manqué (MM).
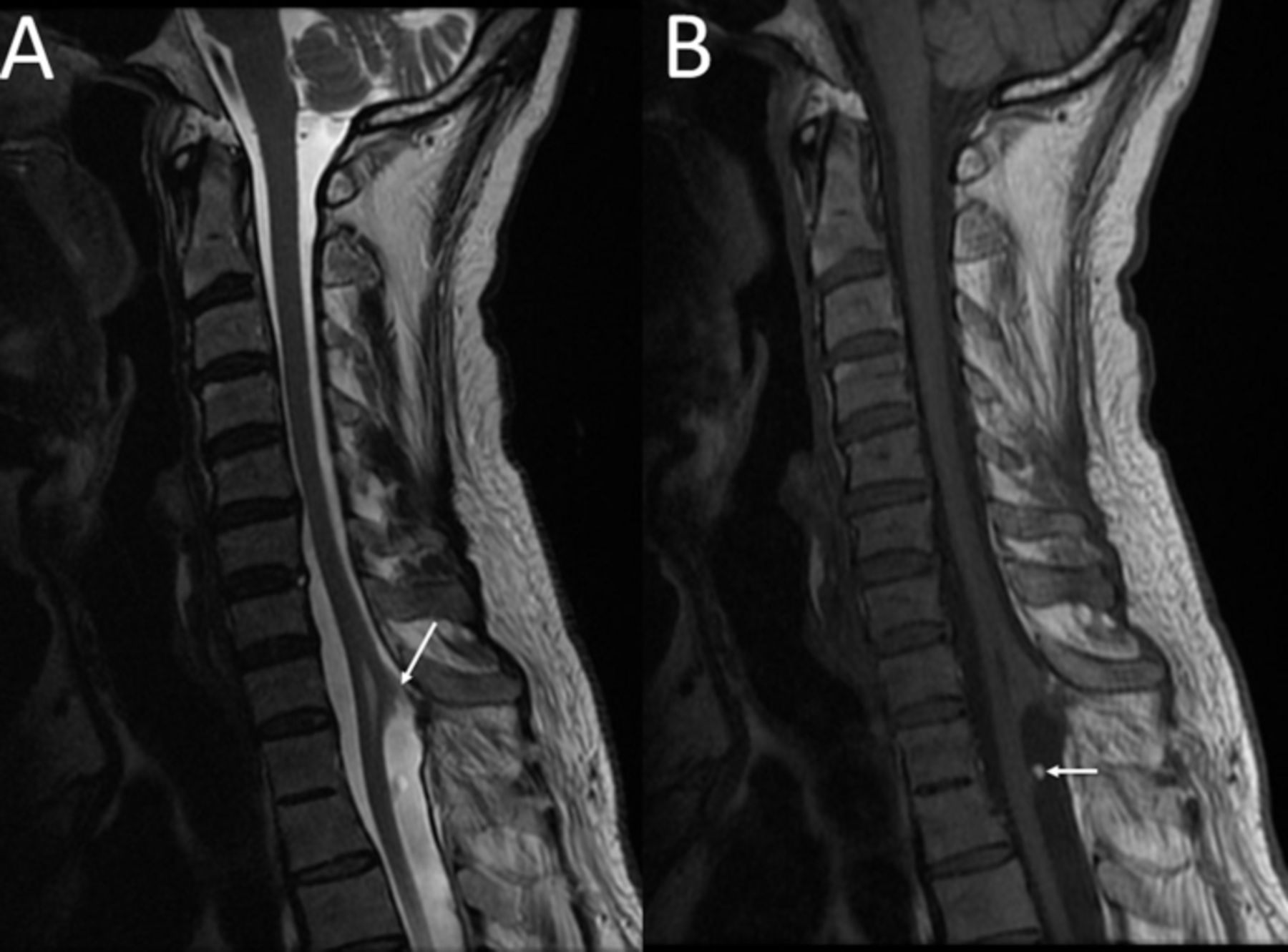
Sagittal T2-weighted (A) and T1-weighted (B) MRI of the cervical spine shows a thin band of tissue tethering the dorsal cord to the dura at T1–2 level (arrow) with resultant formation of a syrinx. At T2–3 level, there is a focal lesion at the dorsal aspect of the thoracic cord with high signal at its tip in keeping with a lipoma of the cord (better appreciated on T1-weighted images—arrow, B). T2–3 vertebrae are also fused in keeping with block vertebrae.

{kind=link}
{kind=link}
Axial T2-weighted (A) and T1-weighted (B) MRI at T1–2 level again demonstrates the band of tissue (arrow, A) extending posteriorly from the dorsal aspect of the spinal cord to the dura in keeping with a meningocoele manqué. Focal dilatation of the central canal of the cord is again noted. The thoracic cord at this level is triangular in cross section. Note is again made of an associated lipoma (arrow, B).
Spinal dysraphism is a broad term which refers to a variety of developmental anomalies occurring in the dorsum of the embryo resulting from abnormal fusion of midline structures.1
Tethered spinal cord syndrome is a type of spinal dysraphism caused by abnormal tissue bands which limit movement of the spinal cord within the spinal column.2 It may be congenital in origin or acquired due to mechanical trauma aggravated by repeated flexion and extension movements or the development of fibrosis in genetically predisposed individuals.
MM has been described as a type of tethered spinal cord caused by fibrous bands or atretic neural tissue to dura or other surrounding structures. It has been diagnosed in neonates; however, it is more commonly found incidentally during investigations for other elements of spinal dysraphism. MRI is considered as the ‘gold-standard’ imaging technique in spinal dysraphisms.3
In our case, the patient was offered corrective surgery; however, he refused and opted for conservative management.
Learning points
Radiological findings of meningocele manqué include fibrous bands causing dorsal tethering of the spinal cord. Associated findings may include lipomas and syrinx formation.
The diagnosis of tethered cord syndrome in adulthood is an unusual but well-described entity.2 The delay in presentation may be associated with the accumulation of microtrauma caused by repetitive spinal flexion and extension.
Surgical intervention may be offered to all symptomatic patients and to asymptomatic patients who lead physically active lives.2
Footnotes
Contributors The MRIs were seen and reported by GG and by RG. AA came across the images while completing her radiology rotation under the supervision of RG and GG.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.