Article Text

Statistics from Altmetric.com
- Cardiovascular medicine
- Contraindications and precautions
- Clinical diagnostic tests
- Radiology (diagnostics)
- Cardiothoracic surgery
Description
A 73-year-old woman with hypertension and atrial fibrillation presented with head and neck injury after mechanical fall. During workup, chest X-ray anteroposterior view (figure 1) revealed a rounded opacity silhouetting the left heart border and hilum. Subsequent contrast-enhanced CT of the chest showed single, 6.4 cm, rounded, well-defined, thin-walled, non-enhanced, low attenuated (−20 and 20 Hounsfield Unit) and homogenous cyst-like structure at the left mediastinum connected to pericardial recesses and not attached to adjacent structures (figure 2A–C). Transthoracic echocardiogram ruled out left ventricular aneurysm, aortic aneurysm, solid tumour and outflow tracts obstruction. Although bronchogenic cyst, oesophageal duplication cyst, thymic tumour and mediastinal lymphoma were considered as possible differentials, radiological features such as CT appearance, homogenous attenuation, unrelated to the underlying structures favoured pericardial cyst. Since patient was asymptomatic, patient and family member were unwilling to undergo surgical removal and pathological confirmation. Follow-up with non-enhanced CT of the chest after 6 months (figure 3A,B) redemonstrated stable size left pericardial cyst. Patient was uneventful at 3 and 6 months follow-ups.

Chest X-ray (anteroposterior view) shows radio opaque left hilar shadow (arrow).
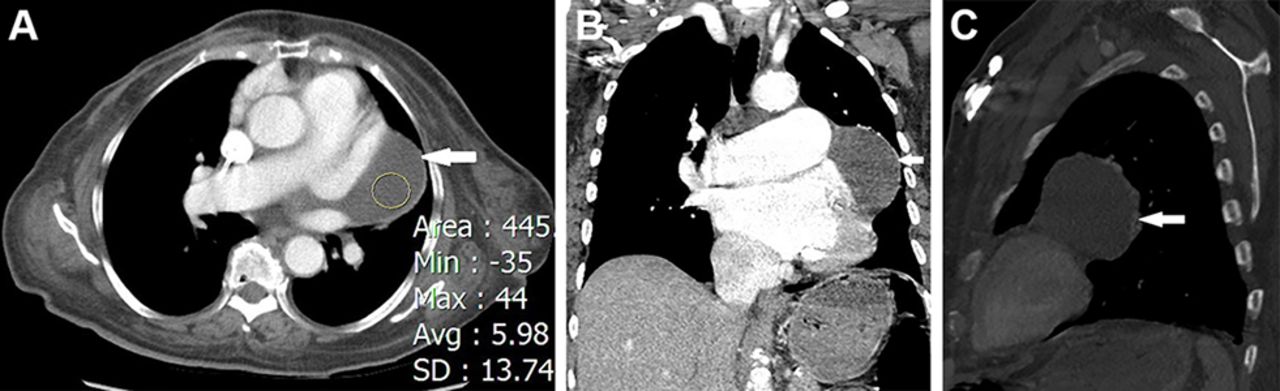
(A–C) Contrast CT angiography of the chest shows well-defined, low attenuated, non-enhanced pericardial cyst (arrow). Cross-sectional plane (A), coronal plane (B) and sagittal plane (C).

{kind=link}
{kind=link}
{kind=link}
(A and B) Non-contrast CT chest after 6 months redemonstrated unchanged size of pericardial cyst (arrow). Cross-sectional plane (A) and coronal plane (B).
Pericardial cyst or mesothelial cyst is a rare benign primary pericardial lesion with estimated incidence of 1:100 000. It results from the congenital malformation of the somatic cavity and defected fusion of parietal recesses. It is discovered incidentally at the cardiophrenic angle, 2/3 on right and 1/3 on left but can be found anywhere in mediastinum.1–4 Approximately, 70% of the cases are asymptomatic but can rarely present with vague symptoms of compression to adjacent structures including cough, shortness of breath, chest pain and arrhythmias. Serious complications such as infection, vascular erosion, ventricular outlet obstructions or sudden cardiac death are extremely rare. Finding of single, well-defined, non-enhanced, low attenuated lesion in typical location and unrelated to surrounding structures in contrast CT or MRI can be useful for diagnosis and for follow-up.5 Conservative management is appropriate in most cases. Surgical interventions are curative but are reserved for the complicated cases, atypical location or doubtful diagnosis.1–6
Learning points
Pericardial cysts are rare and can be incidental finding on imaging.
CT or MRI has been used for diagnostic and follow-up.
To acknowledge management options of pericardial cysts.
Footnotes
Contributors ANL was involved in the conception of the idea, manuscript preparation, patient care and assay analysis.
SL was involved in the patient care and manuscript preparation.
KL was involved in the manuscript preparation, correlative assays and interpretation.
FR was involved in the conception of the idea, patient care and proof-reading.
All the authors approved the submitted manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.