Article Text

Statistics from Altmetric.com
Description
A man aged 33 years presented with a 10-year progressive history of difficulty in walking with poor gripping of flip-flops on feet. It was further associated with foot drop and weakened handgrip. There was a recent history of multiple falls and difficulty in climbing stairs or standing from a squatting position. Family history was suggestive of neurofibromatosis type 1 (NF-1) in grandfather, father, paternal aunt and cousin. Physical examination revealed multiple café-au-lait spots, axillary freckling, Lisch nodules with cutaneous and subcutaneous neurofibromas. On neurological examination, there was spastic quadriparesis with foot drop, distal sensory loss and absent ankle reflexes, which were suggestive of myeloneuropathy. MRI of the cervical spine and whole spine showed characteristic dumbbell-shaped neurofibromas, extending along the Intraspinal and extraspinal areas at multiple cord levels and also along various nerves of the upper and lower limb involving plexuses and roots (figure 1 and figure 2). In view of above clinical and radiological findings, the patient was diagnosed with myeloneuropathy secondary to multiple plexiform neurofibromas. In view of multilevel involvement, orthopaedic and neurosurgical consult was sought but intervention was deemed too risky and thus was ruled out.
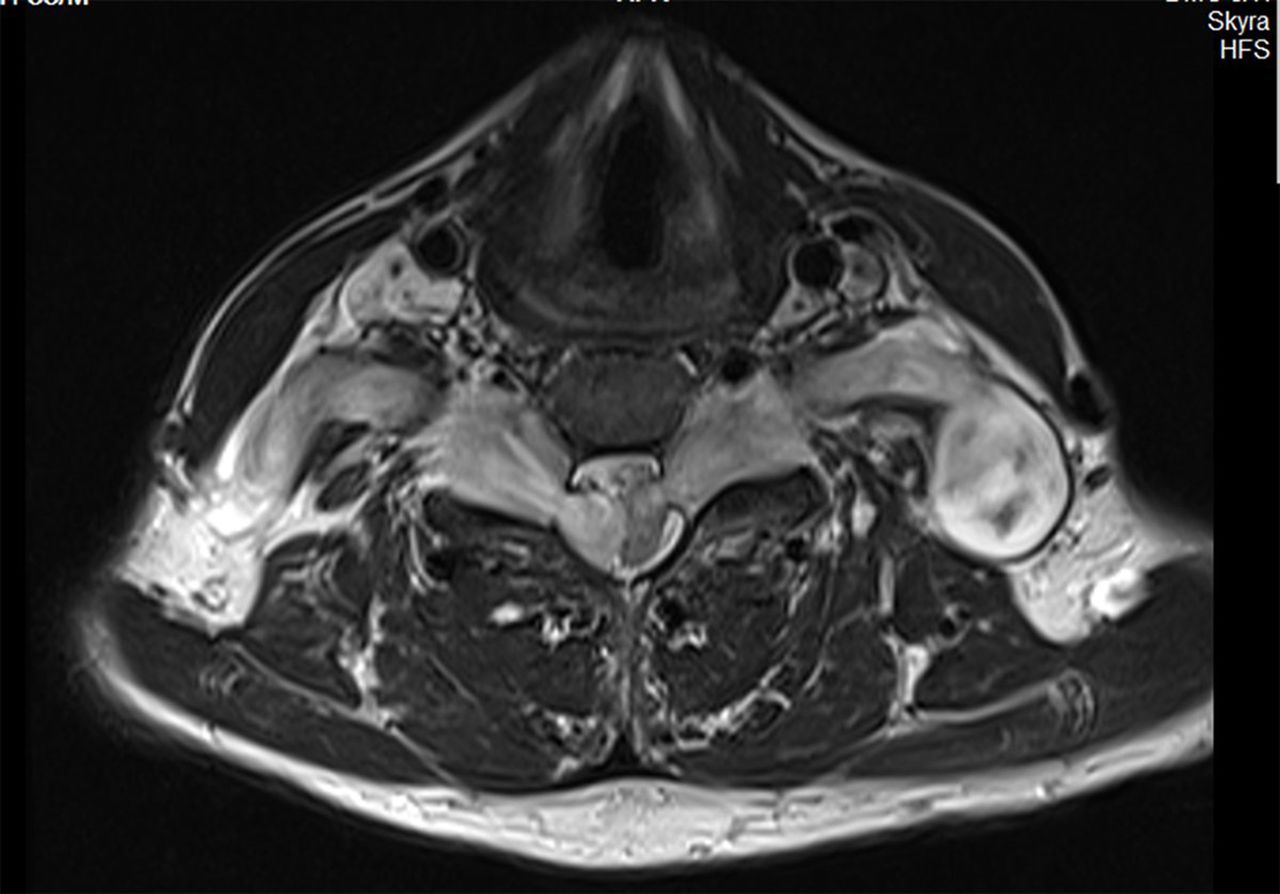
An axial MRI section showing dumbbell-shaped T2 hyperintense lesions seen compressing the cord at C5 level with a hyperintense signal in the cord, suggesting cord oedema.

{kind=link}
{kind=link}
A short tau inversion recovery sequence coronal section of the whole spine. It shows multiple lobulated hyperintense lesions arising from spinal nerves with extradural and intradural component suggestive of dumbbell configuration typically seen with neurogenic tumours.
Cervical cord compression has been described as a rare complication of NF-1 due to cervical root neurofibromas, with quadriparesis being the most common presenting symptom among reported cases.1 Our case highlights the association of plexiform neurofibromas with an unusual presentation of myeloneuropathy due to the involvement of cord as well as multiple nerves, roots and plexuses.
Learning points
Plexiform neurofibromas are commonly associated with neurofibromatosis type 1 (NF-1).
Routine MRI spine screening should be done to diagnose any early nerve, plexus or cord compressions.
One should keep in mind the association of myeloneuropathy with NF-1 when patients present with mixed symptoms of cord as well as neuropathy.
References
Footnotes
Contributors JK conducted acquisition of data and interpretation of data.
BSP did the conception and design.
KS interpreted the data and conducted radiological diagnosis.
JSV designed and structured the report.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.