Article Text

Summary
Abdominal cocoon is an extremely rare condition that has been mainly associated with young adolescent women. It was first described in 1978 by Foo et al. We present here a case that describes an otherwise healthy adult man who presented with intestinal obstruction and was found to have an abdominal cocoon, also known as a peritoneal sac. The patient was taken for a laparotomy and the sac was released through blunt dissection along the avascular planes. He was discharged in good condition 3 days postoperatively. We discuss some of the current literature and previously reported cases on this condition.
- general surgery
- gastrointestinal surgery
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
It discusses and sheds light on a rather rare cause of intestinal obstruction and how to manage it.
Case presentation
A healthy 44-year-old man with no medical or surgical history presented to the Emergency Department with 2 days history of abdominal pain associated with bloating and constipation. There was h/o not passing flatus or motion since morning. Abdominal pain was generalised, and has been progressing in severity and associated with abdominal distension. There was h/o vomiting of 1 episode — the oral contrast. The patient gave a significant history around 1 year back of partial small bowel obstruction that was treated conservatively.
On arrival in the A&E, he was tachycardic with a pulse rate of 111 beats perminute. The patient was well built.
Abdominal examination revealed a distended abdomen that was soft, with no localised tenderness or palpable masses. There was an umbilical hernia defect of 1 cm that was fully reducible. Digital rectal examination showed soft stool, with no blood.
His labs showed the following: haemoglobin 14.9 g/dl, white blood cells 10.7 x10^9/L, neutrophils 8.5 x10^9/L, platelets 283 x10^9/L and C reactive protein 14.5 mg/L. Other lab tests were normal, including renal function tests, lactate and coagulation.
His abdominal x-ray showed hugely dilated small bowel, with air seen in the rectum, consistent with partial bowel obstruction.
He underwent CT abdomen (Figure 1) which showed the following:

CT abdomen, showing dilated small bowel surrounded by a membrane.
‘A sac in the mid-abdomen starting inferior to the SMA. The sac extends to the pelvis and contains mesentry as well as as the distal jejunum and most of the ileum except for the distal 15 cm segment. The bowel loops within it are not dilated. There is mild stranding of the mesentry with streak of free fluid. The proximal jejunal loops are dilated upto 4.5 cm with transition point at the point of sac’.
The impression was an internal hernia as detailed with proximal jejunal obstruction and no signs of ischaemia.
The patient was taken on day 2 of admission for diagnostic laparoscopy + laparotomy + sac release. It was converted to a laparotomy because of the huge multiple compartments, and to avoid any iatrogenic bowel injury.
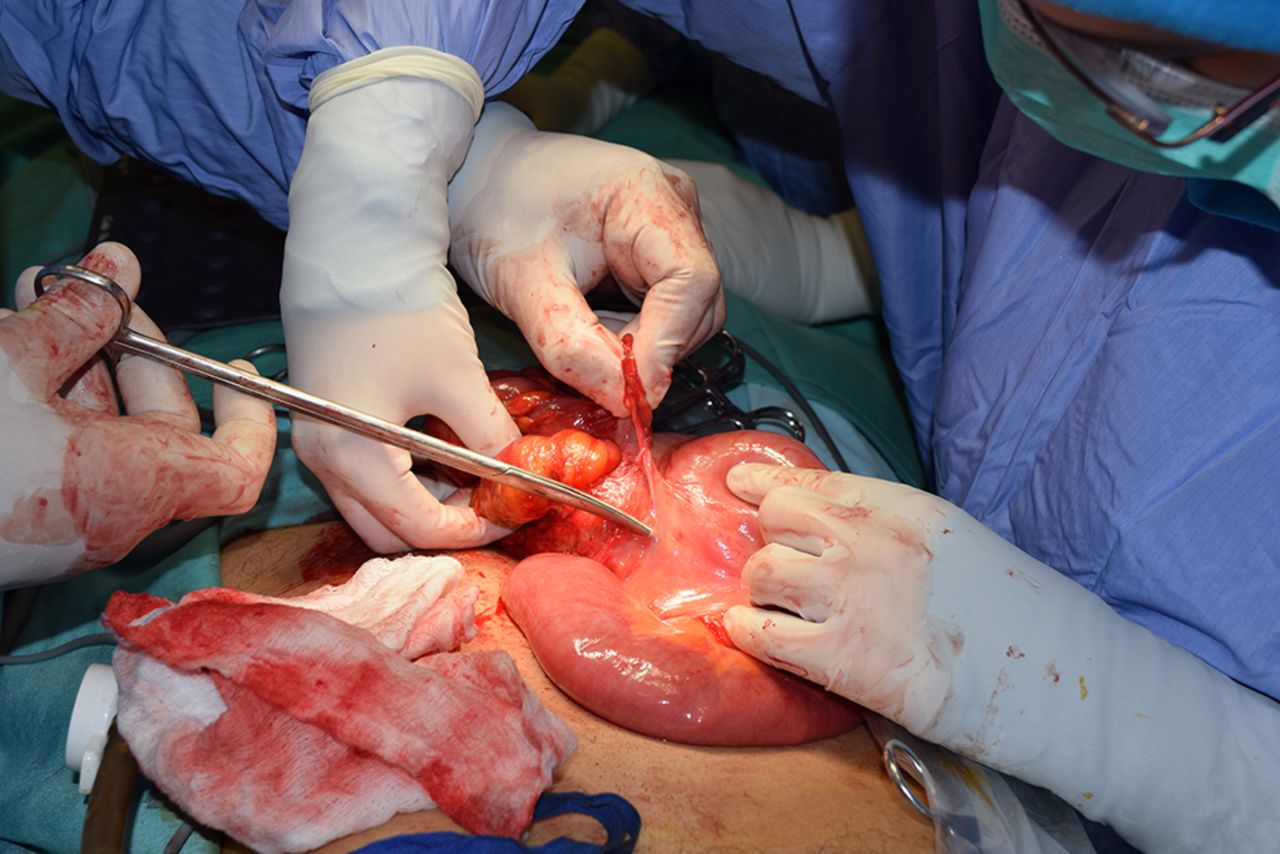
Intraoperative findings were congenital sac seen with multiple compartments that were multilayered, encasing most of the small bowel, and an otherwise healthy small bowel. Figure 2 shows the thin layered sac. Figure 3 shows the multiple compartments. Figure 4 shows the healthy bowel after sac release.

Peritoneal sac is seen as a thin layer.

Small bowel covered by the sac prior to dissection.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The released small bowel looking healthy after dissection.
The%20patient was then discharged on day 3 postoperatively in good condition, and he was then reviewed in the outpatient department on day 11 postoperatively, where he was doing well and with no active issues.
The histopathology examination of the sent specimen showed the following: ‘Cyst wall was compsed of fibrocollagenous tissue with foci of inflammation, haemorrhage and fibrosis. No epithelial lining is seen except in a single loculi, lined by mesothelial cells. No atypical cells or signs of malignancy’.
Outcome and follow-up
The patient was doing well postoperatively and was seen in OPD 2 weeks postoperatively, where he denied any more abdominal pain and has remained asymptomatic.
He was also contacted via phone 3 months postoperatively and was doing well.
Discussion
Abdominal cocoon is an extremely rare cause of small bowel obstruction; it has been reported in previous literature to occur mainly in young adolescent women.1 However, a more recent study done in China showed that abdominal cocoon occurred mostly in Chinese men (87.7%), in the 65 patients who were studied.2
The word cocoon came into English from French, which in turn borrowed it from an Occitan term for ‘eggshell’. The verb ‘cocoon’ has been with us since at least 1881. It is defined as ‘to wrap or envelop in or as if in a cocoon’.3
Abdominal cocoon on the other side was first described in 1978 by Foo et al.4 It refers to a rare condition where there is either total or partial encasement of the small bowel by a fibrocollagenous sac, which looks like a cocoon.1
It is also known to some authors as sclerosing peritonitis, sclerosing encapsulating peritonitis or peritonitis chronica fibrosa incapsulata.4
It has been reported as a disease of unknown pathogenesis that is unique in its feature by packing of the bowel within a dense fibrotic capsule leading to intestinal obstruction.5 It is quite important to differentiate this condition from a congenital peritoneal encapsulation of the small bowel with a thin transparent membrane, which is often found as an incidental finding at laparotomy and almost never causes intestinal obstruction.5
It can be classified as idiopathic or secondary.6 Regarding the causes of idiopathic cocooning, many theories have been postulated, but none have been proven so far.6 One of the commonly known theories that were found in earlier literature was that it was caused by retrograde menstruation with superimposed subclinical peritoneal infection, and that was formulated after noticing the majority of patients were adolescent girls in tropical countries,4 while in secondary abdominal cocoon multiple causes have been reported, including continuous ambulatory peritoneal dialysis, recurrent infective peritonitis, Ventriculoperitoneal shunts, treatment with beta blocker, Tuberculosis, sarcoidosis, familial Mediterranean fever, Systemic Lupus Erythematous, Gastrointestinal malignancies, protein S deficiency and fibrogenic foreign materials.6
In idiopathic abdominal cocoon, the intraoperative finding is that of a thin, easily separated capsule surrounding the small bowel, and as in the presented case can be separated through an avascular plane. In contrast in a secondary abdominal cocoon, it was reported that it was a rather dense fibrous capsule with interbowel adhesions, which are usually quite difficult to separate, as there is no avascular plane.7 This could be explained because of the chronic ongoing infection/inflammatory process, so the sac would be quite adherent.
The condition usually presents with clinical features of acute intestinal obstruction, and patients can give history of previous episodes that have been resolved. Some have been reported to present with a palpable abdominal mass with intestinal obstruction, as in one case reported by Basu et al in Surgery.7 In some studies it was found that the patients who present with idiopathic abdominal cocoon tend to be malnourished, and it was explained to be secondary to anorexia and abdominal pain secondary to recurrent attacks of intestinal obstruction.2
However despite preoperative imaging, diagnosis is done intraoperatively, since imaging can be non-specific. One reported sign on CT is the ‘cauliflower sign’, which is described as a serpentine configuration of dilated small bowel loops in a U-shaped cluster, and delayed transit in a small intestine contrast study is helpful.8 Useful CT and MRI findings are sacculated, dilated bowel loops and soft tissue capsule encircling the bowel loops, which are usually thick on imaging.2 9
One case report done by Ibrahim and Oludara,10 which was published in Tropical Doctor, discussed the management of this condition with surgical excision of the thick membrane, and freeing of the encased small intestine would lead to complete long-term recovery. Bowel is usually viable and resection is not required.
Another study showed that other organs can be encased by the sac (23% of the 65 studied patients); these organs included liver, stomach, appendix, right and left colon, and sigmoid colon.2 Management usually involves the same approach, which is stripping off the membrane.
Recurrence has not been reported, although some patients can present with adhesive intestinal obstruction, in view of all the dissection that has been done. But it usually resolves with the ‘drip and suck’ approach, and one study showed it to be only 6% of the patients.2
Ibrahim and Oludara10 recommend incident appendectomy because the appendix may be difficult to locate if the patient later develops acute appendicitis. But from my point of view now with the expertise in laparoscopic surgery, it is unlikely to be of an issue.
Learning points
CT imaging is an important part of work-up in intestinal obstruction especially in a virgin abdomen.
Surgery is the mainstay of treatment and only involves careful resection of the surrounding sac.
In the case of a peritoneal sac, the small bowel is usually found healthy and no resection is required.
Idiopathic abdominal cocoon is a rare entity that needs to be studied further to know which patients are susceptible to it.
Acknowledgments
The authors would like to thank Dr Sameh Ibrahim and the Colorectal Surgical Team at the Royal Hospital, Oman, and Dr Atheel Kamoona and the Radiology Department at the Royal Hospital, Oman.
Footnotes
Contributors The writing up and the literature review were done by MA-A, while the concept of the paper as well as the revision of the initial submission were done by RA-A. The revised submission was done entirely by MA-A.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.