Article Text

Statistics from Altmetric.com
Description
A 30-year-old primigravida was referred to our institution due to an isolated fetal ascites (IFA). The gestation was uneventful until the 32nd week when the mother was hospitalised due to refractory hypertension. An ultrasound revealed a fetal abdominal circumference above percentile 99. Fetal parameters and amniotic fluid volume were normal.and
The investigation of IFA was started on the mother: blood type was ARh+, indirect Coombs test and infectious serology (toxoplasmosis, syphilis, varicella-zoster, parvovirus B19, rubella, cytomegalovirus and herpes (TORCH)) were negative.
A spontaneous vaginal delivery occurred at 34 weeks. As the ascites compromised ventilation, the neonate was intubated and an urgent paracentesis was performed evacuating 175 mL of a transudate, and thereafter, the caucasian female neonate with 2235 g was stable with spontaneous breathing.
As the ascites persisted, the investigation continued on the neonate: blood group ARh+, negative direct Coombs test and normal echocardiography. Abdominal ultrasound showed dilated bowel loops. The abdominal X-ray revealed three hypertransparent images (figure 1), suggestive of a gastrointestinal anomaly.
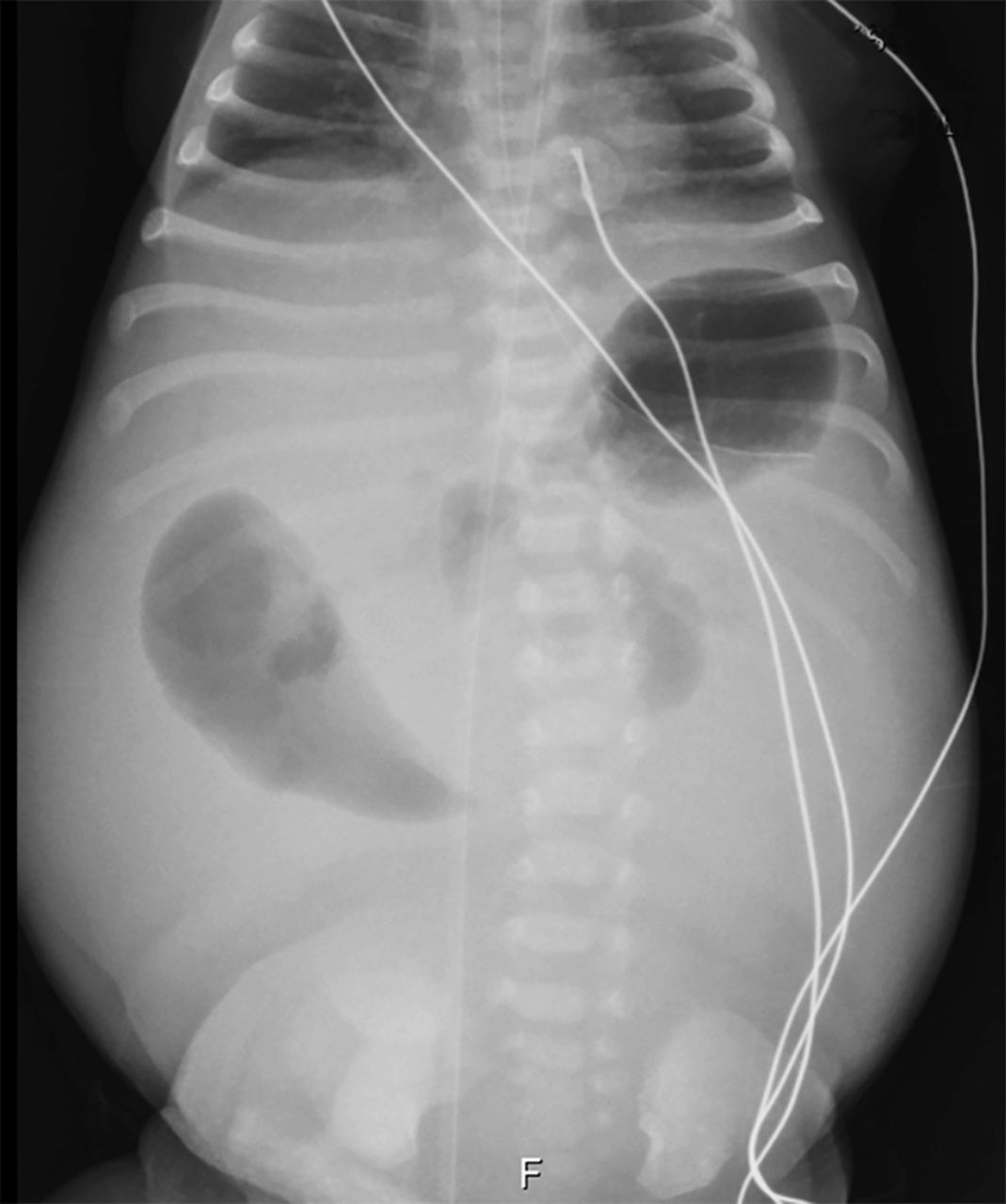
The abdominal X-ray on the first day that revealed three conic hypertransparent images.
On the next day, there was a clinical (figure 2) and radiological worsening (figure 3). So an exploratory laparotomy was performed. A mesenteric defect, with intestinal malrotation and internal hernia was diagnosed. After surgery, she had a significant ponderal loss with a slow weight gain. The screening for cystic fibrosis (CF) was positive (ΔF508 homozygous).

Clinical worsening at day 2 of life: abdominal distension and collateral vasculature.

{kind=link}
{kind=link}
{kind=link}
Radiological worsening at day 2 of life: (A) dilated bowel loops and (B) absence of air in the inferior portion of the abdomen.
At 3 months, she was discharged and referred to CF centre.
IFA is a condition with heterogeneous aetiology: isoimmunisation, congenital infections, chromosomopathies, cardiac, genitourinary and gastrointestinal malformations.1–3 CF has been associated with gastrointestinal anomalies that manifest as IFA.1 Nevertheless, we think this is the first case relating CF with congenital mesenteric defect.
Learning points
When ascites is identifiable in fetal period, the investigation should start in the mother with blood group test, indirect Coombs test, amniocentesis and screening of G6DP deficiency,thalassaemia and TORCH infections. If the ascites persists after birth, the search for an aetiology should continue in the infant with blood group test, direct Coombs test, karyotype, echocardiography, abdominal X-ray and ultrasound.1 3
The cases of isolated fetal ascites (IFA) should be referred to a hospital with tertiary centre. At birth, due to the ascites, ventilation of these neonates can be compromised, so an urgent paracentesis will be needed in the delivery room.
If the cause of IFA is an abdominal anomaly, cystic fibrosis should be always a diagnosis to consider.1
Footnotes
Contributors All the authors conducted the analysis of the described case; RES drafted the manuscript; RAM, SV and JS critically reviewed the manuscript. All authors read and approved the final version.
Competing interests None declared.
Patient consent Consent obtained from guardian.
Provenance and peer review Not commissioned; externally peer reviewed.