Article Text

Statistics from Altmetric.com
Description
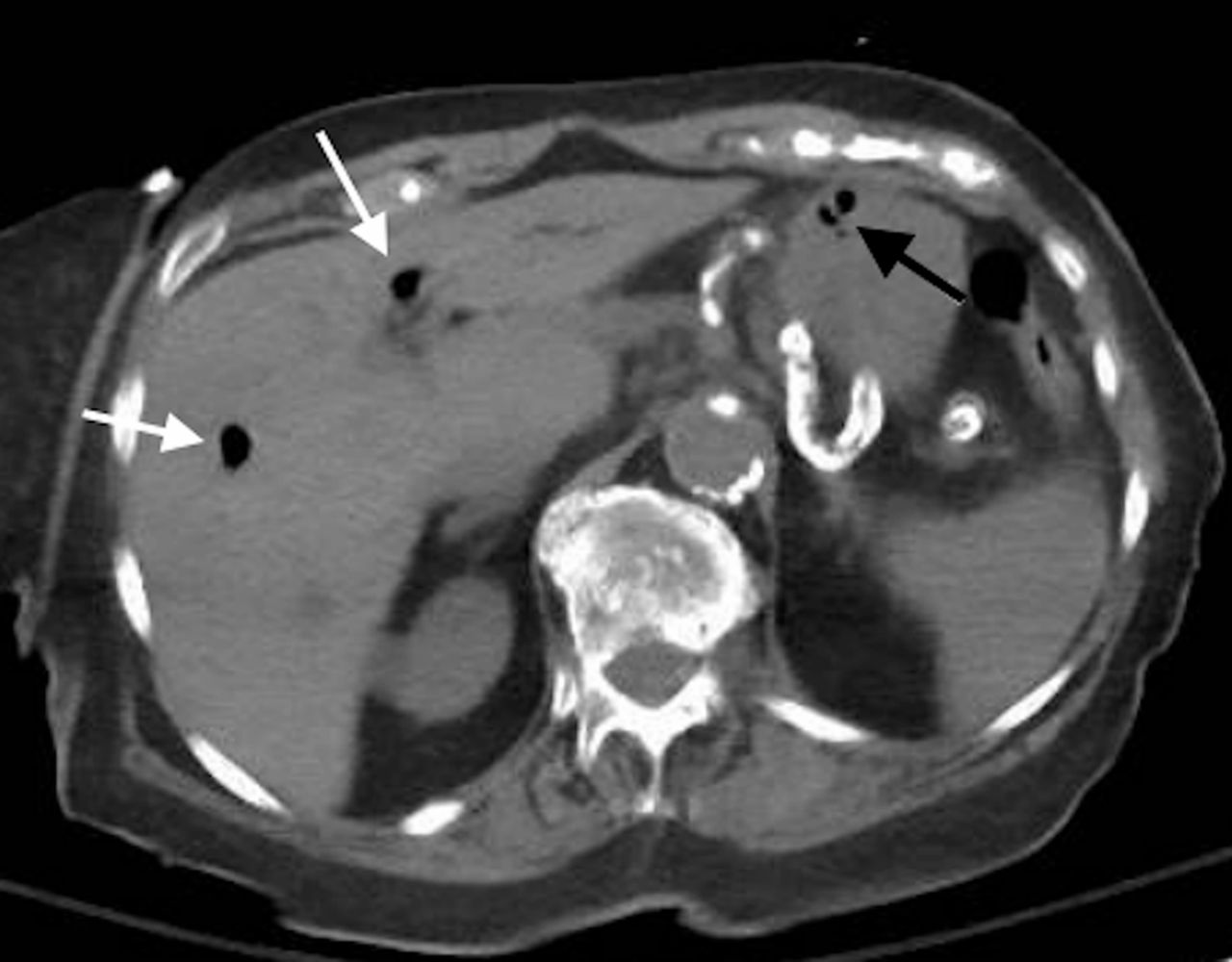
A female aged 94 years with a history of diabetes presented with acute onset abdominal pain, haematemesis and altered mental status. She denied alcoholism, corrosive ingestion, pancreatitis or abdominal trauma. She appeared toxic and was hypotensive. Her hemogram showed leucocytosis at 14.8 x 10^9/L. CT scan of the abdomen showed air scattered within the liver, portal vein and gastric wall (figures 1 and 2). Also, dense calcifications of the aorta and abdominal arteries were noted (figure 3). Due to the high risk of surgery, she was managed conservatively with proton pump inhibitors, broad-spectrum antibiotics, nasogastric decompression and intravenous hydration, with progressive improvement noted.

Axial CT scan of the abdomen and pelvis without contrast showing air within the portal vein (white arrows) and in the stomach wall (black arrow).

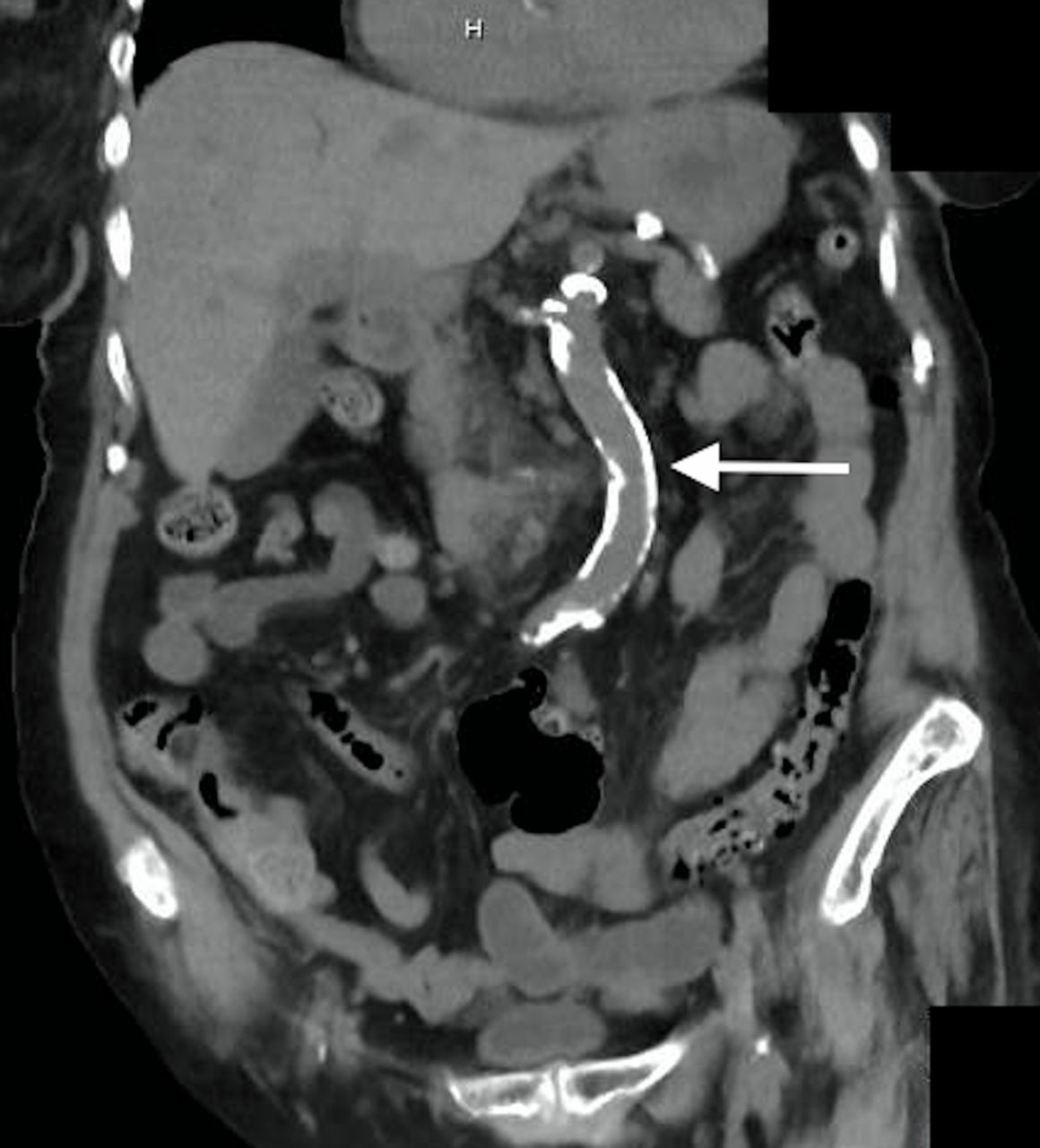
Coronal CT scan of the abdomen and pelvis without contrast showing air within the portal vein (white arrows) and in the stomach wall (black arrow).

{kind=link}
{kind=link}
{kind=link}
Coronal CT scan of the abdomen and pelvis without contrast showing dense calcifications of the aorta (white arrow).
Gastric wall gas is a rare finding secondary to two major diagnosis: gastric emphysema and emphysematous gastritis. The latter is a rare form of gastritis due to the invasion of the gastric wall by gas-forming organisms.1 Given the high mortality of emphysematous gastritis, early recognition and institution of appropriate antibiotics, intravenous hydration and adequate nutrition are key to achieve a positive outcome.
Air within the gastric wall with concomitant portal venous system gas, hypotension, haematemesis and leucocytosis all support the diagnosis of emphysematous gastritis. The aetiology in our case is likely gastrointestinal necrosis caused by severe atherosclerosis as evidenced by her CT scan. Ischaemia increases the risk of gastric wall damage and ulcerations and subsequent invasion by gas-forming organisms.
There has been a trend towards conservative management2 with more recent reports showing improved survival.3 Surgery is only recommended in case of perforation, strictures and uncontrolled sepsis.
Learning points
When air in the stomach wall is found, early differentiation between gastric emphysema (mortality rate of 60%–80%) and emphysematous gastritis (excellent prognosis) is crucial to prevent further complications.
Clinically, patients with emphysematous gastritis present with severe abdominal pain, haematemesis, fevers and leucocytosis in contrast to patients with gastric emphysema who are non-toxic appearing and usually asymptomatic.
Radiologically, CT scan remains the best imaging modality to distinguish between both entities, as air within the stomach wall has a streaky and linear consistency in emphysematous gastritis compared with round air bubbles in gastric emphysema.
Footnotes
Contributors FN and KR drafted the manuscript and acquired the data. IN supervised and critically reviewed the manuscript.
Competing interests None declared.
Patient consent Consent obtained from next of kin.
Provenance and peer review Not commissioned; externally peer reviewed.