Article Text

Statistics from Altmetric.com
Description
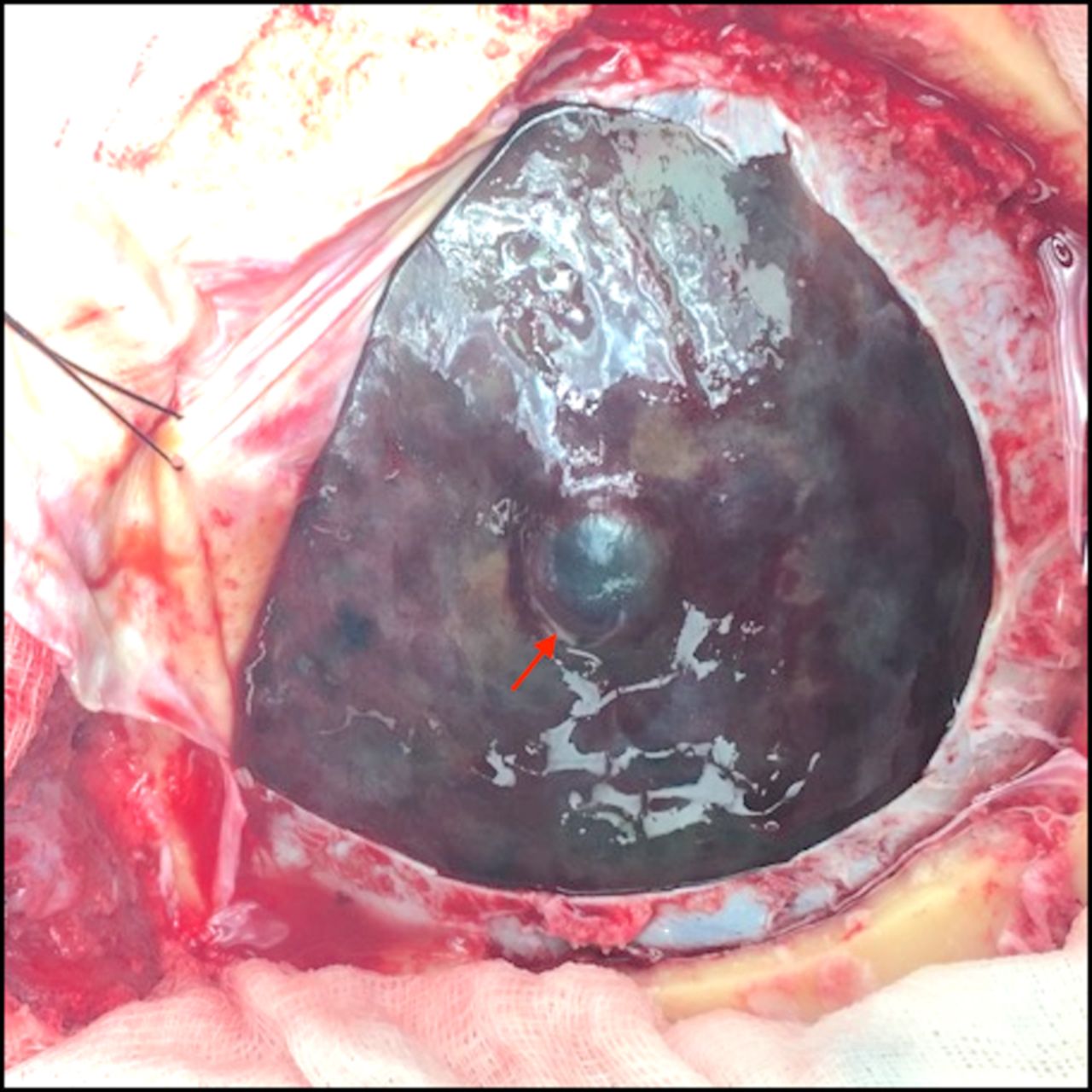
A right-handed man aged 79 years presented with increasing confusion following a mechanical fall with head strike 2 weeks prior. CT demonstrated a left frontoparietal convexity subacute subdural haematoma (SDH) measuring 3 mm in depth and with 5 mm of midline shift to the right (figure 1). There was no skull fracture. Initial examination revealed no localising neurological deficit and he was admitted for observation. On day 3, the patient developed intermittent episodes of right-sided weakness and expressive dysphasia. Contrast MRI showed expansion of the SDH to 10 mm in thickness, and also demonstrated a 9 mm vividly enhancing focus within the haematoma overlying the frontal lobe (figure 2). The lesion enhanced on the arterial and venous phases of contrast CT (figure 3). Digital subtraction angiography demonstrated the lesion to be a 6 mm sidewall aneurysm of the cortical middle cerebral artery (MCA) (figure 4). Craniotomy was performed, the aneurysm trapped and excised with preservation of distal blood flow, and the SDH evacuated (figure 5). Histology demonstrated a lack of a tunica media or adventitia, consistent with pseudoaneurysm. The patient had mild residual weakness but otherwise recovered well and was transferred for rehabilitation.

Initial CT of the brain at presentation showing the left subacute subdural haematoma.

Contrast MRI at day 3 with enlarged subdural haematoma, and enhancing aneurysm (arrow).

(A) Arterial and (B) venous phases of contrast-enhanced CT of the brain demonstrating aneurysm.
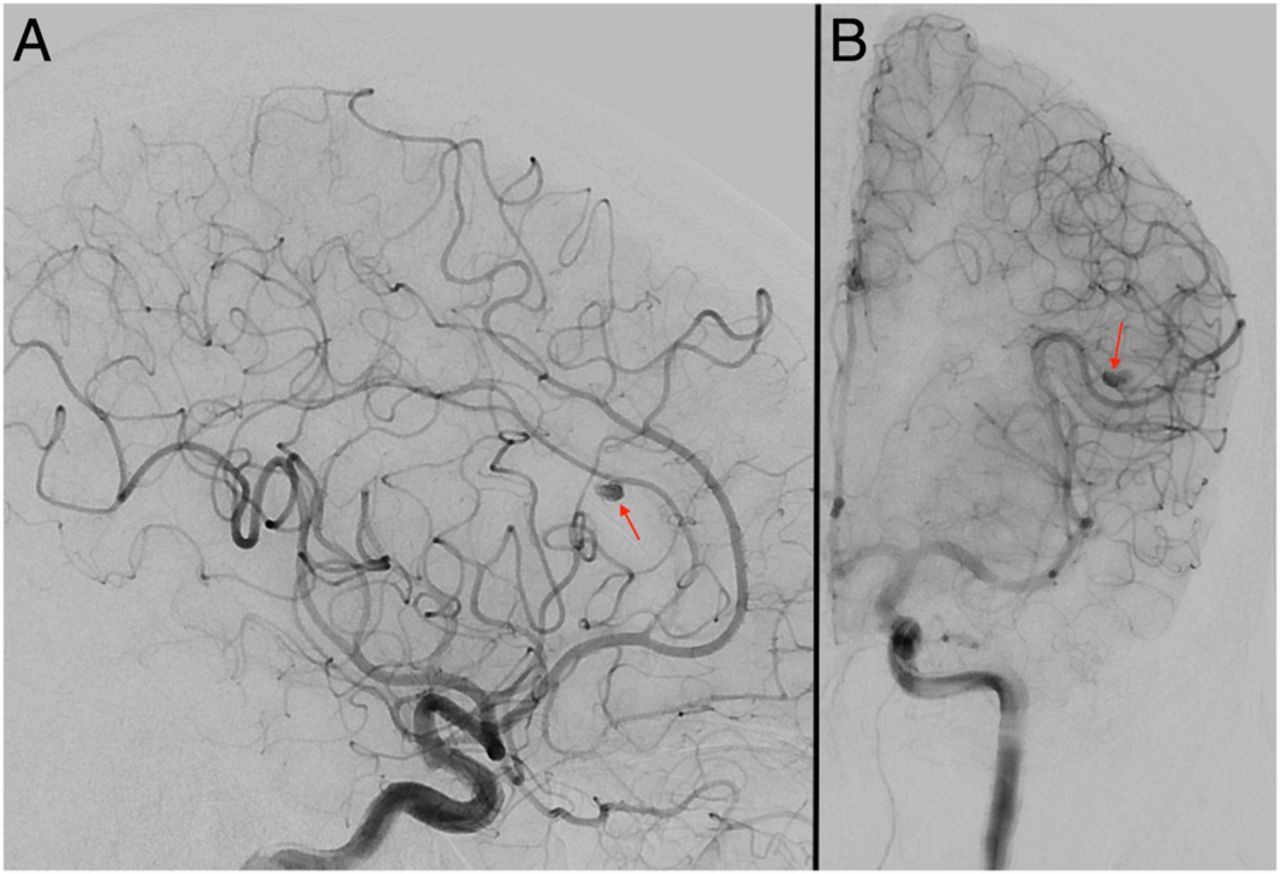
(A) Lateral and (B) anterior–posterior views of a sidewall middle cerebral artery aneurysm (arrows) seen during digital subtraction angiography.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Intraoperative appearance of aneurysm (arrow) seen following durotomy.
Traumatic intracranial aneurysms (TICA) account for only 1% of intracranial aneurysms, but are important because of their propensity to cause delayed bleeding. Several mechanisms can result in TICA, including closed blunt head trauma, missile injury, penetrating injury and iatrogenic injury.1 The average time from traumatic injury to haemorrhage from a TICA is ∼21 days, and in those with ruptured aneurysms, mortality has been reported to approach 50%.2
Traumatic middle cerebral artery aneurysms (TMCAA) are a subtype of TICA and in 93% of cases occur in the cortical segment of the MCA, usually in association with skull fracture.3 Owing to their location, 55% of TMCAA present with SDH.3 About 83.3% are pseudoaneurysms resulting from complete transmural injury of the artery.2 ,3 In a review of 28 cases of 32 traumatic MCA aneurysms, delayed rupture occurred in 46.7% of patients, an average of 4.7 days following injury.3 Two patients in this review had multiple TMCAA; all were ipsilateral and were found along linear parietal bone skull fractures. TMCAA are usually amenable to surgical trapping and excision without compromise of distal bloodflow.3
Patients with delayed neurological deterioration following head injury should undergo cerebral angiography to investigate for TICA, and if found, early surgical intervention is recommended to prevent rebleeding.
Learning points
Traumatic middle cerebral artery aneurysm (TMCAA) can occur following head trauma, and rupture of the aneurysm can result in subdural haematoma.
TMCAA can cause delayed bleeding, manifesting as new neurological deficit some days following head injury.
TMCAA can be effectively treated with surgical trapping and excision without compromising distal blood flow.
Footnotes
Contributors LB, PS and SV contributed equally to the composition of this ‘Images in…’ Case Report. All three were involved in the direct clinical care of the patient described, and the authors subsequently shared the load of review of clinical material, writing, figure creation, editing and review.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.