Article Text

Statistics from Altmetric.com
Description
Ascending aorta pseudoaneurysm is a high-risk complication post cardiac surgery.1 Although surgical repair is the conventional method of treatment, it is associated with a high mortality rate of 30% and a very poor prognosis.2 We report an old man aged 85 years who underwent elective biological aortic valve replacement for severe aortic valve stenosis and closure of left atrial appendage with AtriClip. Cardiopulmonary bypass was established with standard ascending aorta and right atrial cannulations. The aortic valve was replaced with 27 mm Hancock II type using 2/0 Ethibond pledgetted sutures in interrupted suture techniques. His medical history included arterial hypertension and atrial fibrillation on rivaroxaban. Despite uneventful postoperative recovery and no symptoms at his follow-up, he presented 4 months later with sternal tenderness and soft tissue swelling at the midpart of sternotomy wound; oral antibiotic was started at that stage and he was discharged home. Two months later, he was referred to the cardiothoracic surgery unit with a sticky dark blood stained discharge from the same swelling with stable sternum.
A suspicion of ascending aortic pseudoaneurysm was confirmed with an urgent contrast chest-CT scan. This showed a large retrosternal haematoma and a 22 mm pseudoaneurysm arising from the ascending aorta above the non-coronary cusp of the prosthetic aortic valve (PAV) without any other pathological findings (figures 1⇓–3, video 1).
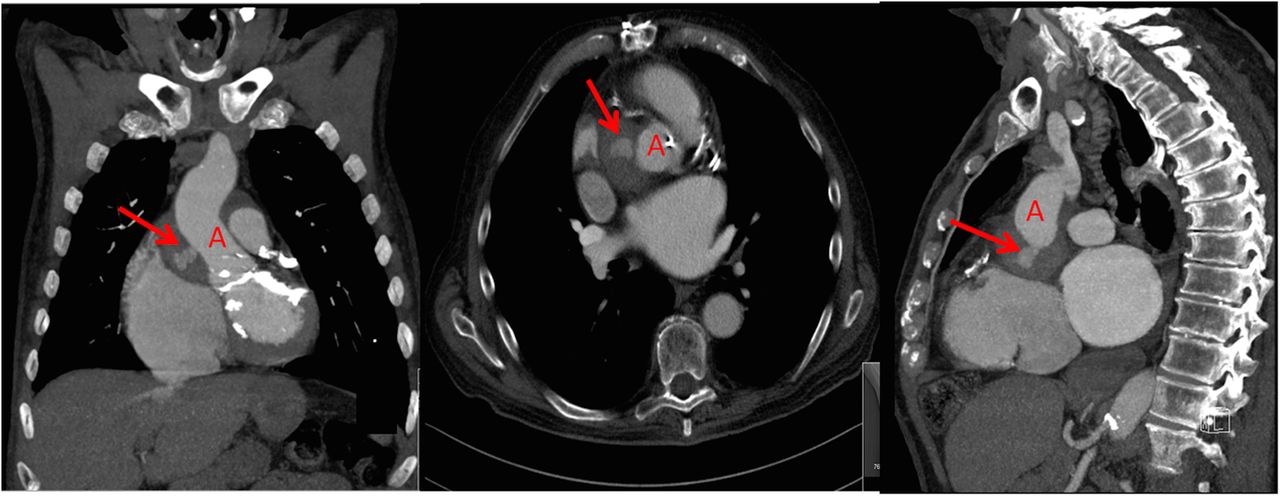
Enhanced contrast CT scan of the thorax showing pseudoaneurysm (arrow) arising from the ascending aorta (A).

Three-dimensional reconstruction of CT thorax showing the pseudoaneurysm behind the right atrium (RA). RCA, right coronary artery.

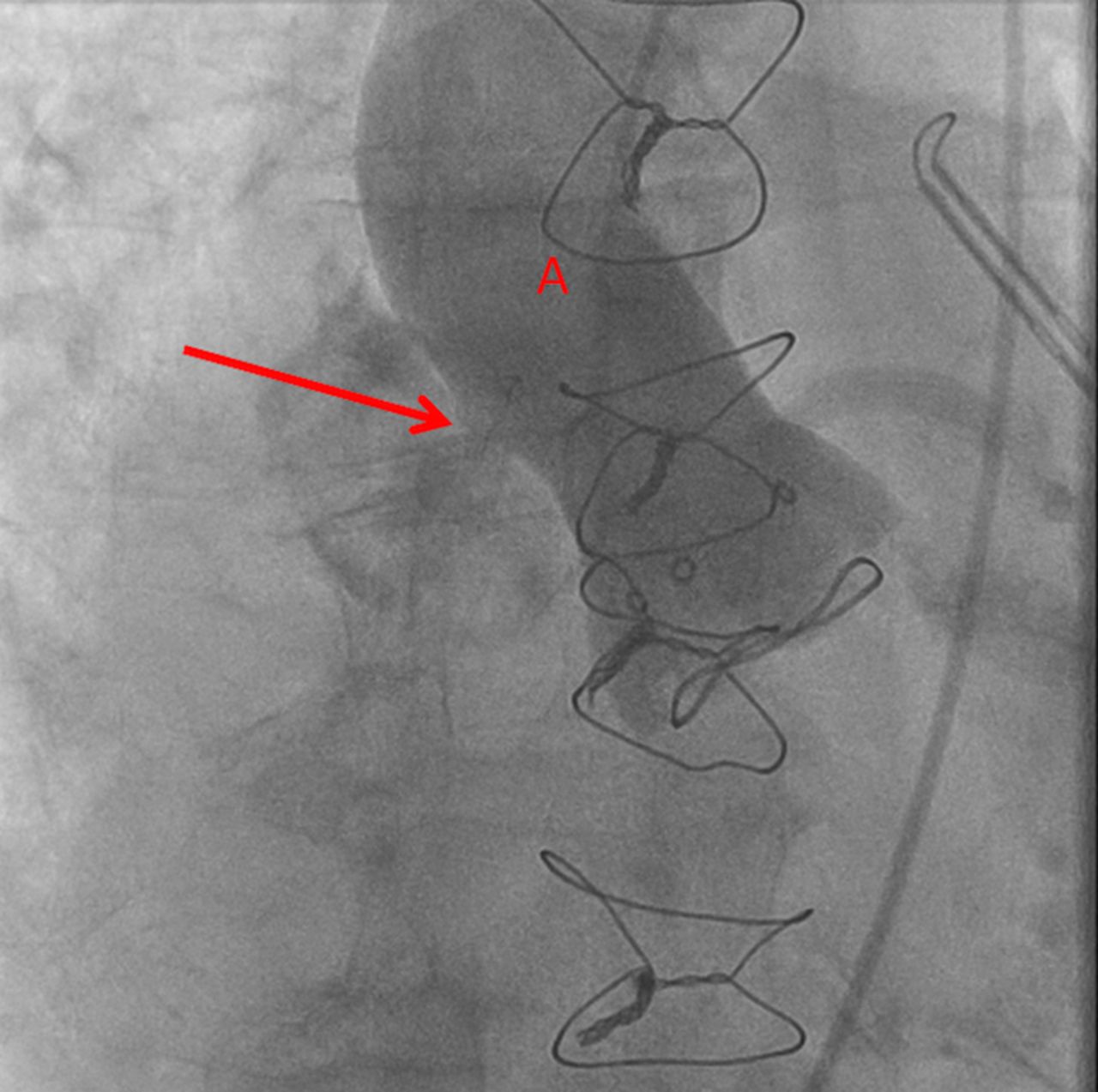
Intraprocedure angiogram showing location of the pseudoaneurysm (arrow) arising from the ascending aorta (A).
Pseudoaneurysm of the ascending aorta prior to device deployment.
After discussion in multispecialty team meeting, a non-surgical treatment was advised. Because of the proximity of the pseudoaneurysm to PAV, a percutaneous closure was preferred to endovascular aortic repair. This was performed successfully in a hybrid cath-laboratory using a 6 mm Occlutech device (figure 4, video 2). Repeated contrast CT aortogram confirmed complete closure of the pseudoaneurysm (figure 5). The patient was discharged home early in good health with significant improvement of the sternal tenderness and swelling.
Learning points
Postoperative sternal wound complications should be taken into serious consideration and early referral to the cardiothoracic surgical unit is highly recommended.
Late heavily blood stained sternal wound discharges should raise the suspicion of retrosternal bleeding or collection.
Non-surgical approach is recommended for treatment of aortic pseudoaneurysm post cardiac surgery.
Intraprocedure angiogram showing successful closure of the pseudoaneurysm (arrow) that arise from the ascending aorta (A).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Contrast CT scan of the thorax showing successful occlusion of the pseudoaneurysm (arrow) that arise from the ascending aorta (A).
Successfully occluded pseudoaneurysm.
Footnotes
Contributors AH and AK prepared and reviewed the manuscript, JC provided the necessary images for the case report and reconstructed the 3D images. SK is the responsible cardiac surgeon who operated on the patient.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.