Article Text

Statistics from Altmetric.com
Description
A 57-year-old man presented to the emergency department with fever, chills and a wound on his left foot since 2 weeks. He had no previous medical history. Despite receiving flucloxacillin, the wound was neglected and became necrotic with skin discoloration and a purulent, foul-smelling discharge. The leg developed functional impairment with severe claudication pain. All digits were pale, cold and numb (figure 1A, B). Biochemistry showed high infection parameters and hyperlactaemia as a sign of hypoperfusion. Hyperglycaemia revealed de novo diabetes. X-rays of the left lower extremity showed subcutaneous air (figure 2A–C).

(A,B) The extension of necrotising fasciitis of the left lower extremity.

X-rays of the foot (A) and knee (B and C) showing subcutaneous air (arrows), which is typical of necrotising fasciitis.
Patient underwent immediate left transfemoral amputation. Postoperatively he was treated in the intensive care unit with piperacilline/tazobactam and clindamycin due to septic shock. Microbiological cultures revealed a Bacteroides fragilis and Pasteurella species. Histology confirmed necrotising fasciitis (figure 3A–C). CT angiography showed a stenosis in the common and left external iliac artery for which a stent was placed by percutaneous transluminal angioplasty (figure 4). Patient recovered and was discharged to a rehabilitation centre.
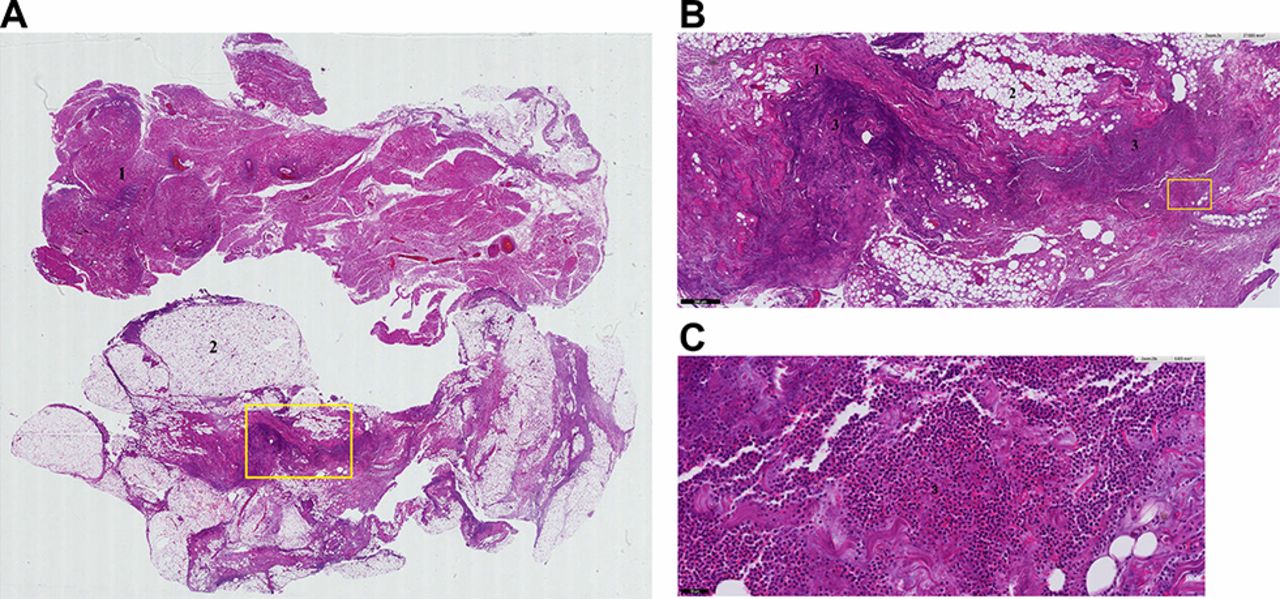
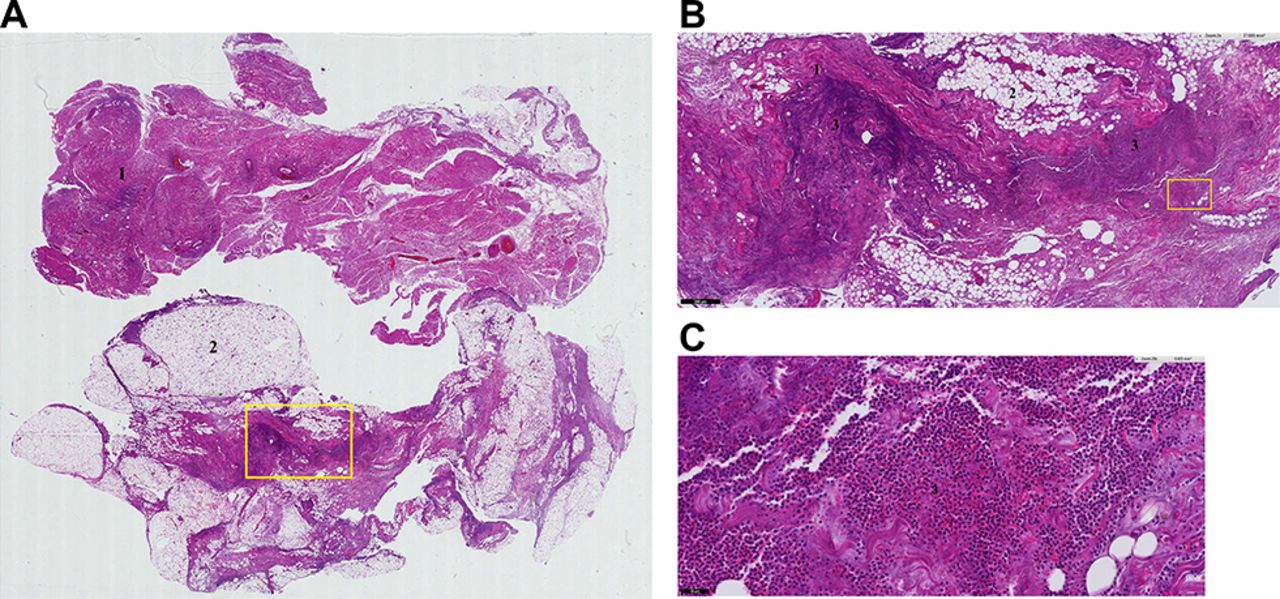
(A) Overview of tissue from the left lower extremity affected by necrotising fasciitis showing fascia (1) and fat tissue (2). (B) The infiltrate (3) is localised next to the fascia (1). (C) The infiltrate (3) contains neutrophils, which implies bacterial infection. A pathology analysis contributes to the clinical diagnosis of necrotising fasciitis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CT scan showing a stenosis (arrow) of the common and external left iliac artery left.
This case illustrates that delayed recognition and treatment can cause rapid disease progression and increases the risk of a poor outcome. It is characterised by inflammation, sepsis, multiorgan failure and even death, with a mortality rate of 30%.1 2 There are many risk factors for development of necrotising fasciitis (box). Necrotising fasciitis is polymicrobial in nature, with most cultures yielding a mixture of aerobic and anaerobic organisms (table 1). Early diagnosis of necrotising fasciitis and aggressive treatment with surgical debridement and antibiotics determine its outcome.3 Despite excellent healthcare in developed western countries, a fulminant course of necrotising fasciitis with disabling outcomes can still occur.
Risk factors for necrotising fasciitis
Immunosuppression: medication (such as steroids, chemotherapy, infliximab) or disease (AIDS, malignancy, tuberculosis) induced
Cardiovascular diseases: arteriosclerosis, congestive heart failure, renal failure
Trauma: fractures, surgery, insect/animal bites, frostbite, intravenous drug abuse
Skin diseases: systemic lupus erythematosus, abscess, psoriasis, varicella
Gastrointestinal: diverticulitis, perirectal abscess or perforated viscus
Other: diabetes mellitus, obesity, pregnancy, advanced age
Bacteria causing necrotising fasciitis
Learning points
Provide adequate instructions to patients with wounds in order to prevent unnecessary extension and impairment; especially in patients with risk factors, such as diabetes and smoking.
Necrotising fasciitis is an uncommon but potentially fatal condition especially if unrecognised.
Management should consist of immediate resuscitation, early surgical debridement and administration of broad spectrum intravenous antibiotics.
Footnotes
Contributors KvS is responsible for admitting the patient to the hospital, participated i
n writing the article (and revision), and received informed consent from the patient.
CS is responsible for care of the patient in the ICU and participated in writing the article
(and revision). DHTT is responsible for care of the patient in the ICU and critically revised
the article. RM is responsible for surgical care of the patient and critically revised the article. KvS and CS are guarantors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.