Article Text

Statistics from Altmetric.com
Description
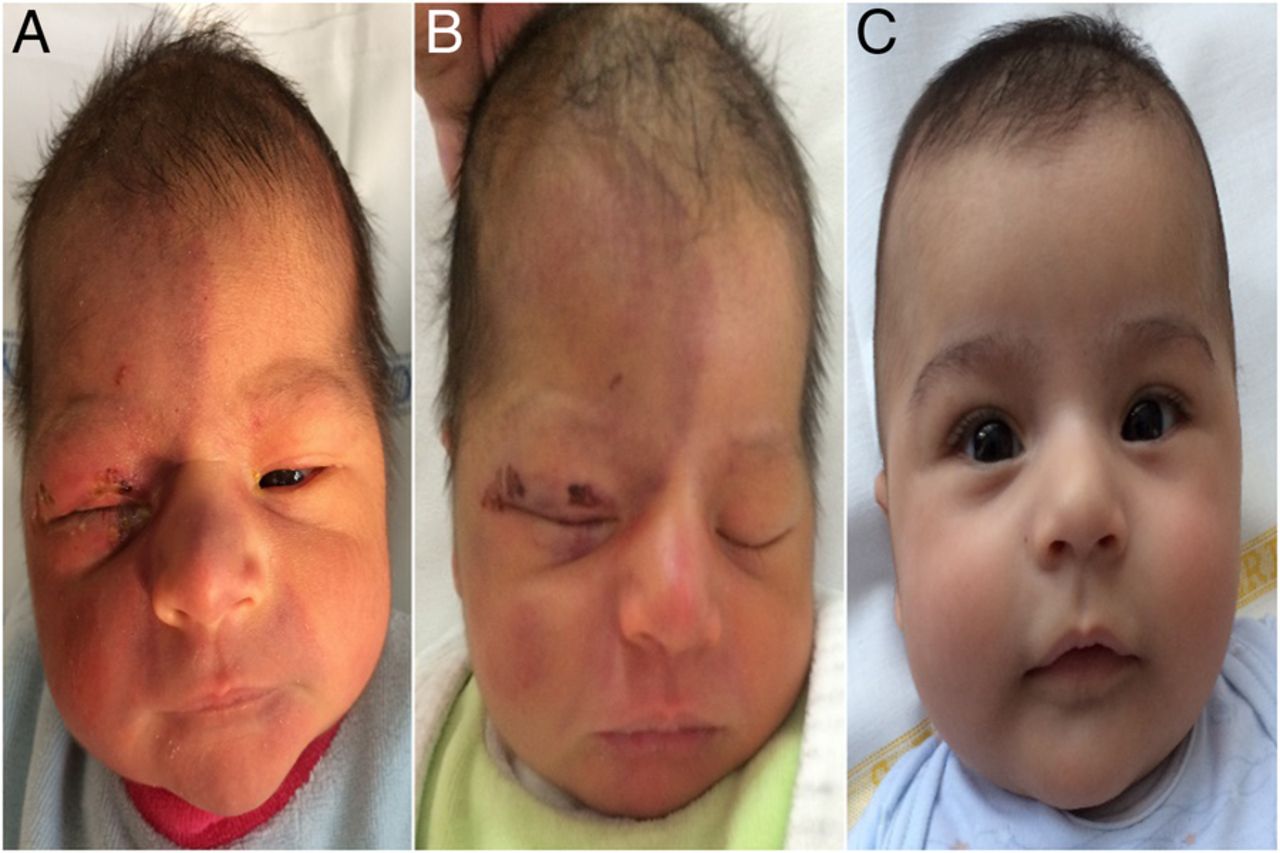
A few hours after birth, a newborn was admitted to Santobono-Pausilipon III level Hospital. Suspected eye injury was reported. During childbirth, the baby showed a face presentation and to help with the delivery, a vacuum extractor (VE) method was used. Body weight of the baby at the time of birth was 3200 g, length 50 cm and head circumference 35 cm. Apgar scores were 7I and 8V. The newborn was subjected to examinations by an ophthalmologist and a neurologist and tested by a CT. The ophthalmological examination of the right eye revealed an extensive conjunctiva haemorrhage, dioptric media was transparent, anterior chamber was normal, optical disc had defined margins and retinal haemorrhages were absent. A neurological examination reported extensive haematoma of the right half-face and excoriations of the right eyelid (figure 1A, B). Bregmatic fontanelle was normotensive, archaic reflexes were present and symmetrical. CT scan results confirmed the absence of damage on the right eye or nerve. The infant's wound was treated with betamethasone–chloramphenicol ointment applied four times a day, mupirocin ointment three times a day for a total of 9 days with good results (figure 2A, B). Follow-up to 3 months showed complete recovery of the infant without sequelae (figure 2C). Childbirth with a face presentation ranges from 0.5 to 3 per 1000 deliveries; its cause and mechanism are not yet understood.1 The use of VE presents higher rates for traumatic and non-traumatic intracranial haemorrhages compared with infants born by caesarean section (CS) or by a non-assisted vaginal delivery.2 Therefore, the use of VE method has been proven high-risk procedure, CS choice should be considered.3

(A, B) Lesions at the time of admission.

{kind=link}
{kind=link}
(A) The lesions after 6 days of therapy and (B) after 9 days of the therapy. (C) Follow-up at 3 months from discharge.
Learning points
The use of vacuum extractor presents higher rates of complications compared with caesarean section (CS).
CS should be considered in cases of face presentation.
Footnotes
Contributors GDB made substantial contributions to the conception of the work and acquired data. MS analysed and interpreted data with GDB. GDB, MS and MG drafted the work. MG and DS revised it critically for important intellectual content.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.