Article Text

Statistics from Altmetric.com
Description
A man aged 15 years was referred to the otolaryngology department with a 5-year history of persistent nasal blockage and nocturnal mouth breathing. He did not report any additional sinonasal, aerodigestive tract or neurological abnormalities. Flexible nasendoscopic examination revealed adenoidal hypertrophy occluding the choanae bilaterally.
Adenoidectomy by monopolar suction diathermy under direct visualisation was performed. Following adenoidectomy, intraoperative visualisation of the surgical site revealed a well-circumscribed left of midline soft tissue swelling of the posterior pharyngeal wall.
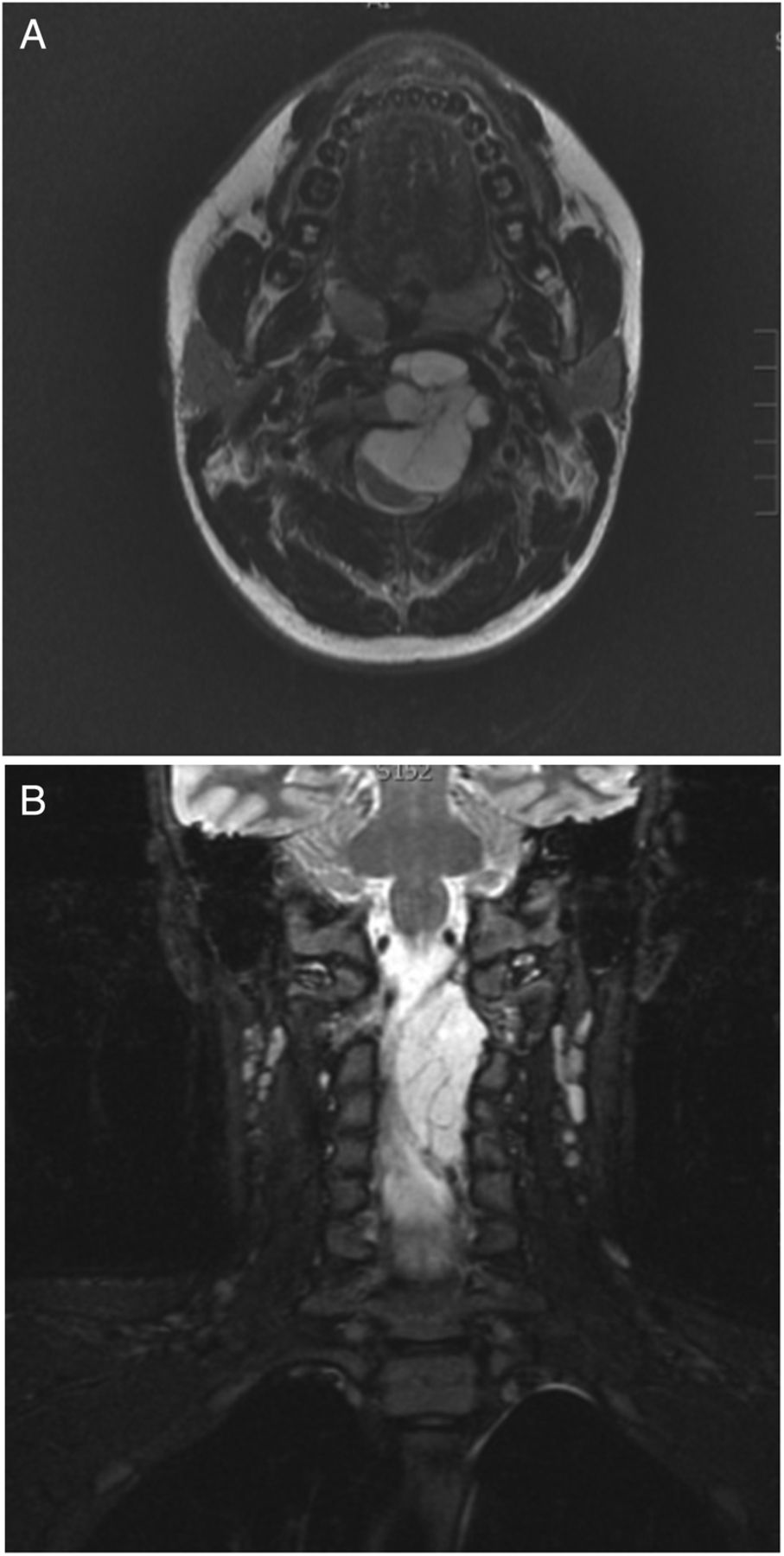
Postoperative MRI illustrated a destructive lesion arising from the left C2/3 nerve root with extracanalicular and intracanalicular components, the latter of which was causing severe cervical cord compression (figure 1A, B). The radiological diagnosis was consistent with neurofibroma. The patient was urgently referred to neurosurgery for definitive management. Although asymptomatic, neurosurgical evaluation demonstrated an upper motor neuron syndrome affecting the upper limbs and the left lower limb. Hoffman's sign was present on the left. The patient underwent a cervical laminectomy C2–C4 with resection of the lesion. The final histological diagnosis was chordoma, with no evidence of de-differentiation.

{kind=link}
(A) Axial T2-weighted MRI scan illustrating a lesion arising from the left C2/3 nerve root. (B) Coronal STIR sequences illustrate a lobulated hyperintense mass extending over a distance of 6 cm from the top of the odontoid peg to the C4/5 disc space.
Adenoidectomy is commonly performed via conventional curettage. It is a blind method of removing adenoid tissue transorally relying on digital palpation and surgical experience with peroperative bleeding obscuring the operative field. Alternatively, monopolar suction diathermy involves ablation of adenoids by direct visualisation with an endoscope or laryngeal mirror providing a clear operative view with minimal bleeding.
As described below, in this case, the differential is wide. The initial radiological diagnosis was that of neurofibroma; however, eventual histology confirmed chordoma. This diagnostic difficulty on MRI has been reported in the literature as both chordomas and neurofibromata demonstrate low-to-intermediate T1 and high T2 signal intensity on MRI.1 Chordomas are rare, slow-growing, locally aggressive tumours of notocordal origin that arise along the cranio-coccygeal axis.2 Metastases are rare.3
Learning points
In the paediatric population, nasal obstruction is usually a symptom of common disease processes such as adenoidal hypertrophy, but it should be remembered, as in this case, that the underlying cause may be multifactorial in origin. Nasal obstruction may be the cardinal presenting symptom for more serious underlying pathology.
Visualisation of the nasopharynx at the end of the procedure is crucial for diagnosis of nasal obstruction and complete removal of adenoidal tissue. We would advocate that visualisation with laryngeal mirror or endoscope is good practice when performing adenoidectomy, irrespective of the technique used.
Differential diagnoses of nasopharyngeal lesions include normal anatomical structures, such as adenoidal hypertrophy; benign lesions, such as lipoma and neurofibroma; or malignant lesions, such as rhabdomyosarcoma and lymphoma. Other differentials include those of embryonic origin, such as chordoma; or vascular origin, such as aneurysms of the carotid system.
Footnotes
Contributors CS drafted the original manuscript. PC, AQ and AM provided critical appraisal. All authors approved the manuscript prior to submission.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.