Article Text

Statistics from Altmetric.com
Description
A boy aged 16 years presented to our hospital with a history of dyspnoea on exertion and haemoptysis. His cardiovascular examination revealed features of severe pulmonary artery hypertension (PAH). He had no cyanosis. His transthoracic echocardiogram showed dilated right atrium and ventricle with the interventricular septum bulging to the left side. There was a small perimembraneous ventricular septal defect (VSD) with right-to-left shunt (figure 1 and video 1). The left atrium and ventricle were of normal size. Continuous wave Doppler evaluation showed right-to-left shunting with a peak gradient of 33 mm Hg, thus indicating suprasystemic PAH. Doppler evaluation of the tricuspid regurgitation (TR) jet showed a gradient of 120 mm Hg (figure 2). The pulmonary artery (PA) was hugely dilated with spontaneous echocontrast, but no thrombus (figure 2 and video 2). In spite of extensive evaluation, we could not find a secondary cause for pulmonary hypertension in this patient and PAH was presumed to be idiopathic or primary PAH superimposed on a small VSD. He was treated with a combination of phosphodiesterase inhibitor sildenafil and endothelin inhibitor ambrisentan. Severe PAH has been described in small VSD1 and after spontaneous closure of VSD.2 In those cases, initially, VSD was large enough to initiate pulmonary vascular disease. In our case, we think that the two pathologies are coincidental, as there were no clinical features of a large VSD at any time.

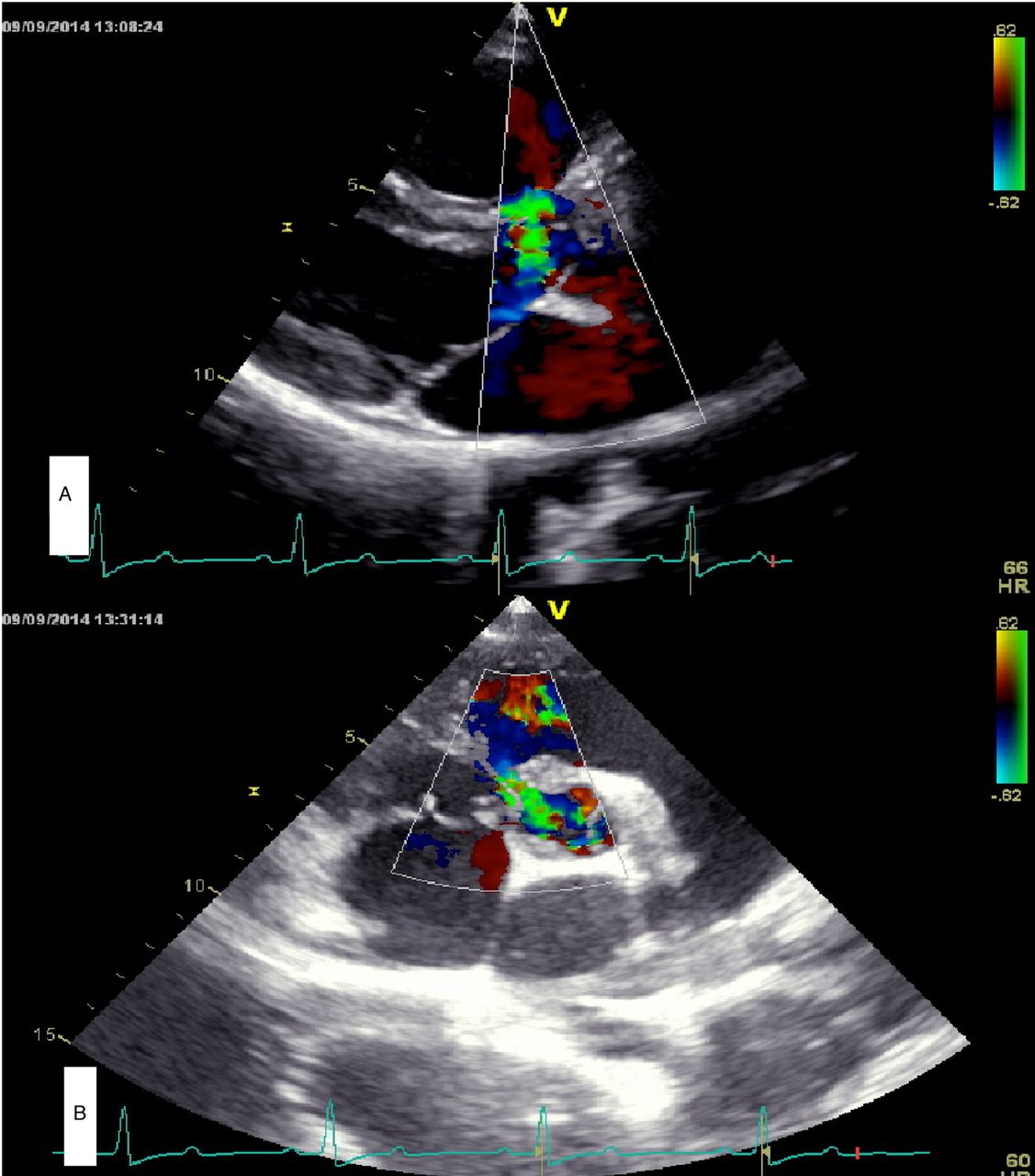
Transthoracic echocardiogram: (A) parasternal long-axis view showing small perimembraneous ventricular septal defect (VSD) and the right-to-left shunt. (B) Parasternal short-axis view showing 2 mm subaortic VSD.

{kind=link}
{kind=link}
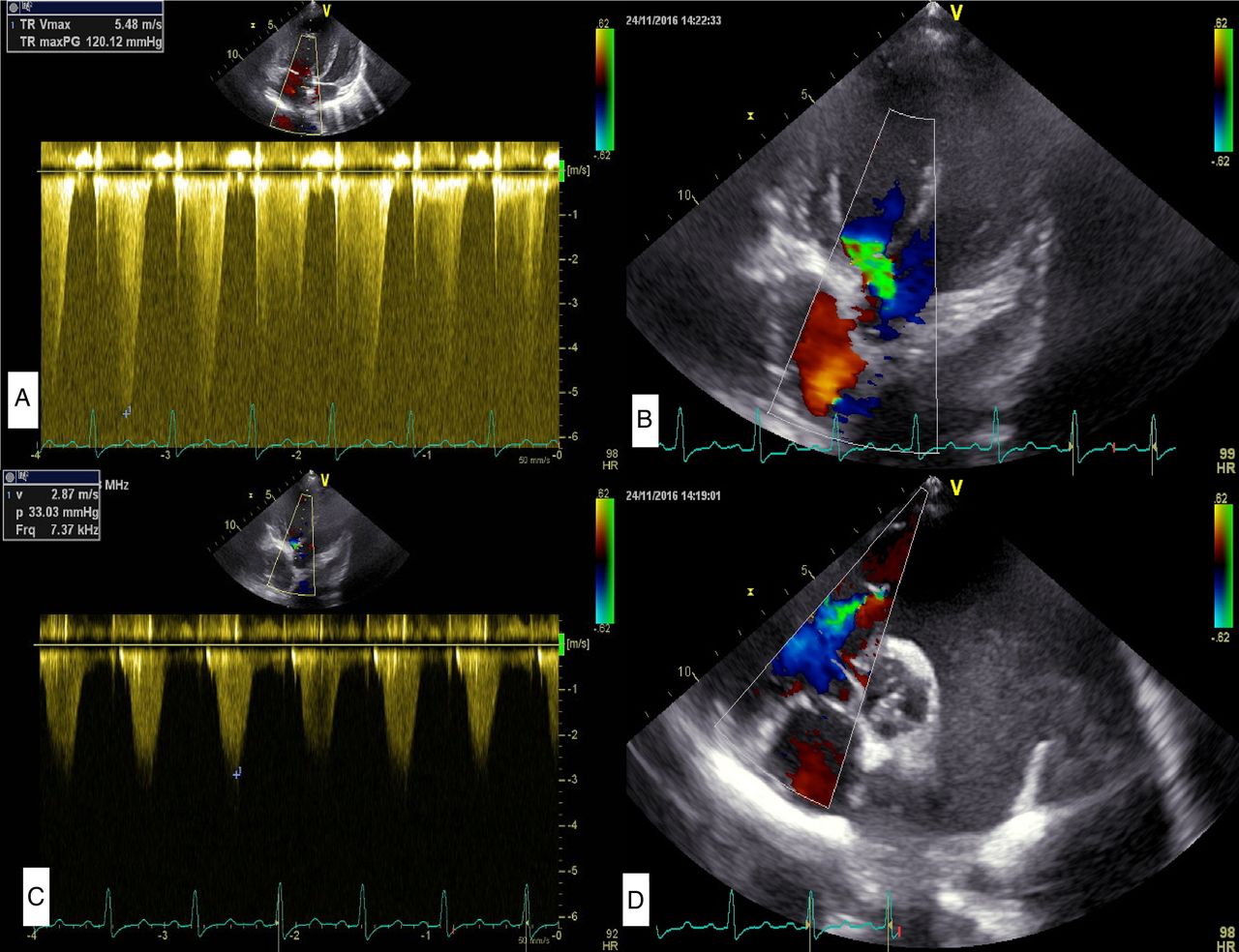
Transthoracic echocardiogram (A) Continuous wave (CW) Doppler evaluation of tricuspid regurgitation (TR) showing TR peak gradient of 120 mm Hg. (B) CW Doppler showing the right-to-left shunt with a gradient of 33 mm Hg. (C) Apical five-chamber view showing the right-to-left shunt. (D) Parasternal short axis showing hugely dilated pulmonary artery with spontaneous echocontrast and pulmonary regurgitation.
Transthoracic echocardiogram apical five-chamber view showing the right-to-left shunt through ventricular septal defect.
Grossly dilated pulmonary artery with spontaneous echocontrast and pulmonary regurgitation.
Learning points
The presence of congenital heart disease may be pathologically irrelevant in many patients as in our case where the lesion is haemodynamically insignificant.
The patient should be evaluated for a secondary cause including thromboembolic pulmonary artery hypertension in such a case.
The velocity and direction of flow across the small ventricular septal defect could actually be useful in monitoring the natural history or response to medication in this patient.
Footnotes
Contributors Both the authors are actively involved in the conception and design, acquisition of data and writing up the manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.