Article Text

Summary
Oral hairy leukoplakia (OHL) is an oral mucosal lesion that is associated with Epstein-Barr virus infection. It commonly presents as an asymptomatic, non-removable white patch on the lateral borders of the tongue in individuals who are immunocompromised. Historically, OHL was thought to be pathognomonic of HIV infection; however, it is now an established phenomenon in a range of conditions affecting immune competence. Hairy cell leukaemia (HCL) is a rare chronic B cell lymphoproliferative disease named after the distinctive cytology of the atypical cells. We report the first case of OHL arising in an individual with HCL that resolved following remission of the haematological malignancy.
Statistics from Altmetric.com
Background
Oral hairy leukoplakia (OHL) is an oral mucosal lesion associated with infection and replication of the Epstein-Barr virus (EBV).1 OHL was first described in 1984 and has largely been reported as an HIV-associated and AIDS-associated condition.2–4 It has, however, also been described in HIV-negative immunocompromised individuals, such as transplant recipients secondary to immunosuppressant medication, patients with haematological malignancies, and more recently in those using inhaled steroids and anticonvulsants.5–8 Therefore OHL is now best regarded as a marker of immunosuppression rather than being pathognomonic of HIV infection.
The characteristic clinical presentation of OHL is that of an asymptomatic, non-removable white patch with a corrugated surface typically involving the lateral and dorsolateral surfaces of the tongue bilaterally. It less commonly occurs in other oral sites such as the buccal mucosa and gingivae.9 The most common histopathological features of OHL include hyperparakeratosis, epithelial hyperplasia, koilocyte-like cells within the prickle cell layer and minimal or complete absence of inflammatory cells in the lamina propria even with the presence of candida on the surface. A band-like layer of cells with clear cytoplasm can also be seen in the upper spinous layer.9 10 These features are not exclusive to OHL, and therefore EBV demonstration in lesional tissue is required for definitive diagnosis.11 12 Various techniques have been described for the detection of EBV in tissue sections, including in situ hybridisation (ISH), PCR and immunohistochemistry.13–15 Due to the abundant expression of EBV-encoded RNA (EBER1 and EBER2) in latently infected cells, EBER is a suitable molecular target for detecting the presence of EBV. Therefore EBER ISH is considered to be the gold standard.11 12 16
Here we describe a case of OHL in association with hairy cell leukaemia (HCL). HCL is a rare chronic B cell lymphoproliferative disease characterised by splenomegaly, pancytopenia and infiltration of leukaemic cells into the liver, spleen and bone marrow.16 HCL derives its name from the distinctive cytology of the atypical cells, which demonstrate surface hair-like projections and membrane ruffles identified in the blood and/or bone marrow.17 Identification of these clinical and morphological features along with identification of a V600E mutation in the BRAF gene, which has been shown to be a reliable molecular marker, is used for diagnosis.18 After a literature search of PubMed and Medline, this is the first time that OHL associated with HCL has been reported in the literature.
Case presentation
A 48-year-old male was referred to the Oral Medicine Department at Bristol Dental Hospital for assessment of an asymptomatic white patch of 6 months’ duration on the right lateral border of his tongue. On initial presentation, there was no significant medical history and the patient was a never-smoker. Extraoral examination of the head and neck was unremarkable, with no evidence of lymphadenopathy. Intraoral examination revealed a relatively extensive soft, slightly raised, corrugated white patch localised to the right lateral border of the tongue (figure 1).

Corrugated white patch on the right lateral border of the tongue.
There was some slight sharpness of the cusps of the lower molar teeth bilaterally, which were thought to be contributing to this lesion. A clinical working diagnosis of frictional keratosis was made, with OHL as a differential. The patient returned to his general dentist for the fabrication of a lower polythene occlusal cover and smoothing of the lower molar cusps, and a review appointment was made 3 months later.
At this follow-up appointment, there had been no change in the appearance of this lesion. There had, however, been a significant change in his medical history. A routine full blood count had been undertaken by his general medical practitioner which identified both neutropaenia (1.07×109) and thrombocytopaenia (75×109). An urgent referral to haematology followed where bone marrow aspirate and trephine biopsy were undertaken, which showed a diffuse infiltrate of medium-sized lymphoid cells with cytoplasmic projections. Molecular analysis of DNA from the bone marrow aspirate also tested positive for the BRAF Val600Glu mutation. These features were all consistent with a diagnosis of HCL.
As a result of this change in medical history, our working diagnosis changed from frictional keratosis to OHL presenting secondary to HCL-related immunosuppression. After liaising with haematology, an incisional biopsy of the lesion was performed with prophylactic antibiotic cover. The patient had a reported penicillin allergy; therefore, it was agreed that clindamycin 600 mg given 1 hour preoperatively followed by 300 mg three times a day for 7 days was the most appropriate. Local measures of cautery and primary wound closure were adopted.
The histopathology revealed mucosa comprising parakeratinised and acanthotic stratified squamous epithelium with surface corrugation. A band of vacuolated cells was seen just beneath the parakeratin layer, and the superficial lamina propria was devoid of any inflammatory cells (figure 2). Periodic acid–Schiff stain revealed the presence of candidal hyphae. EBER ISH was performed and showed numerous positive cells, confirming EBV-related pathology (figure 3). A clinicopathological diagnosis of OHL was made.

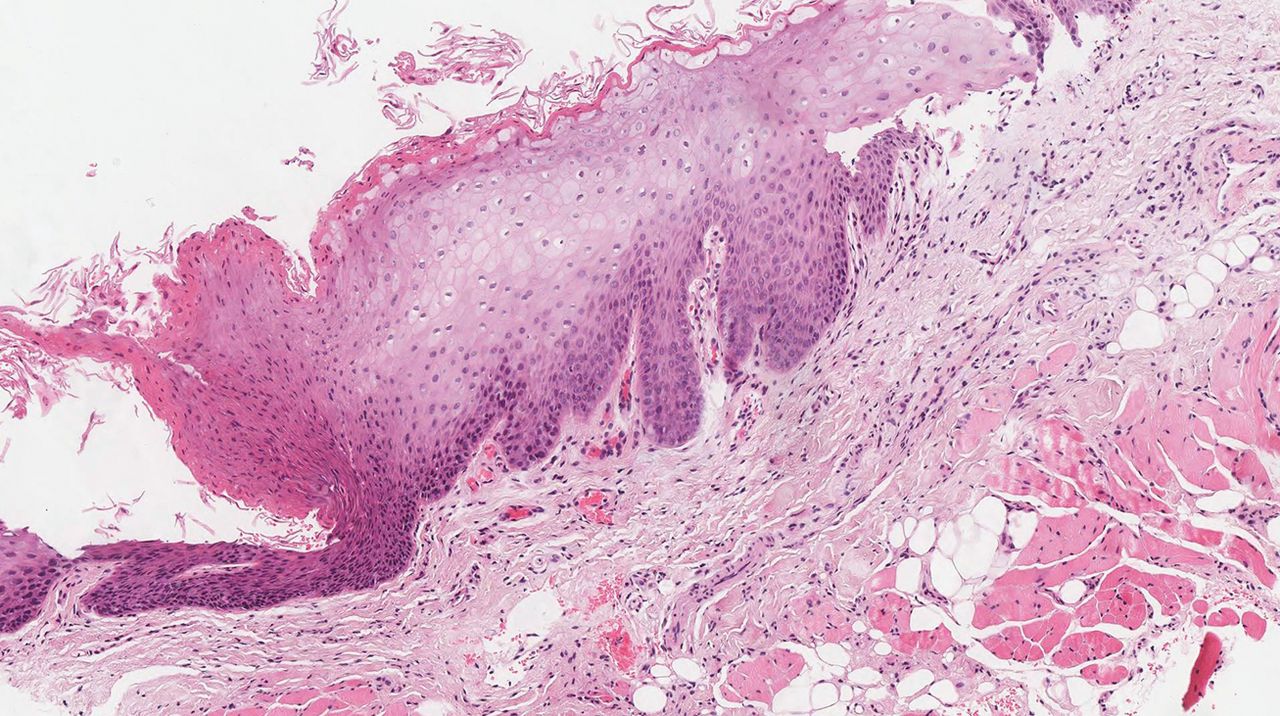
H&E stained section (x10). Epithelium showing hyperparakeratosis, acanthosis and a band of vacuolated cell. No significant inflammatory cell infiltrate is seen in the underlying lamina propria.
{kind=link}
{kind=link}
{kind=link}
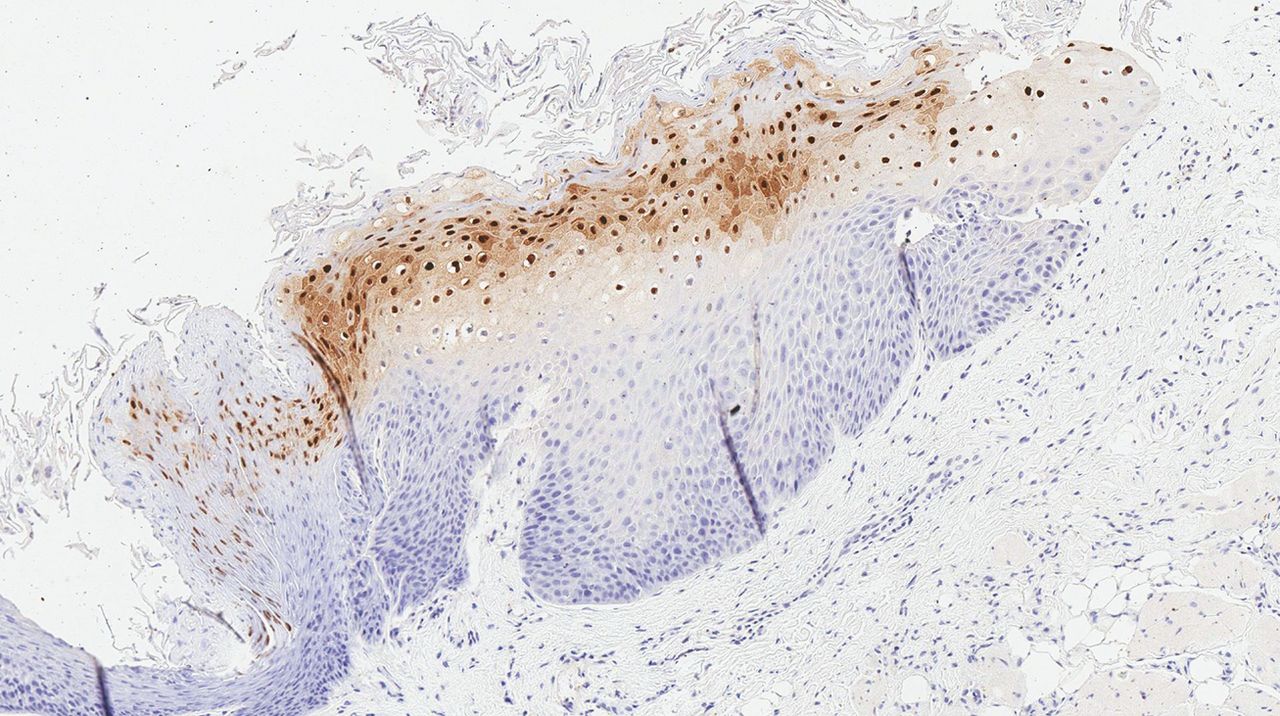
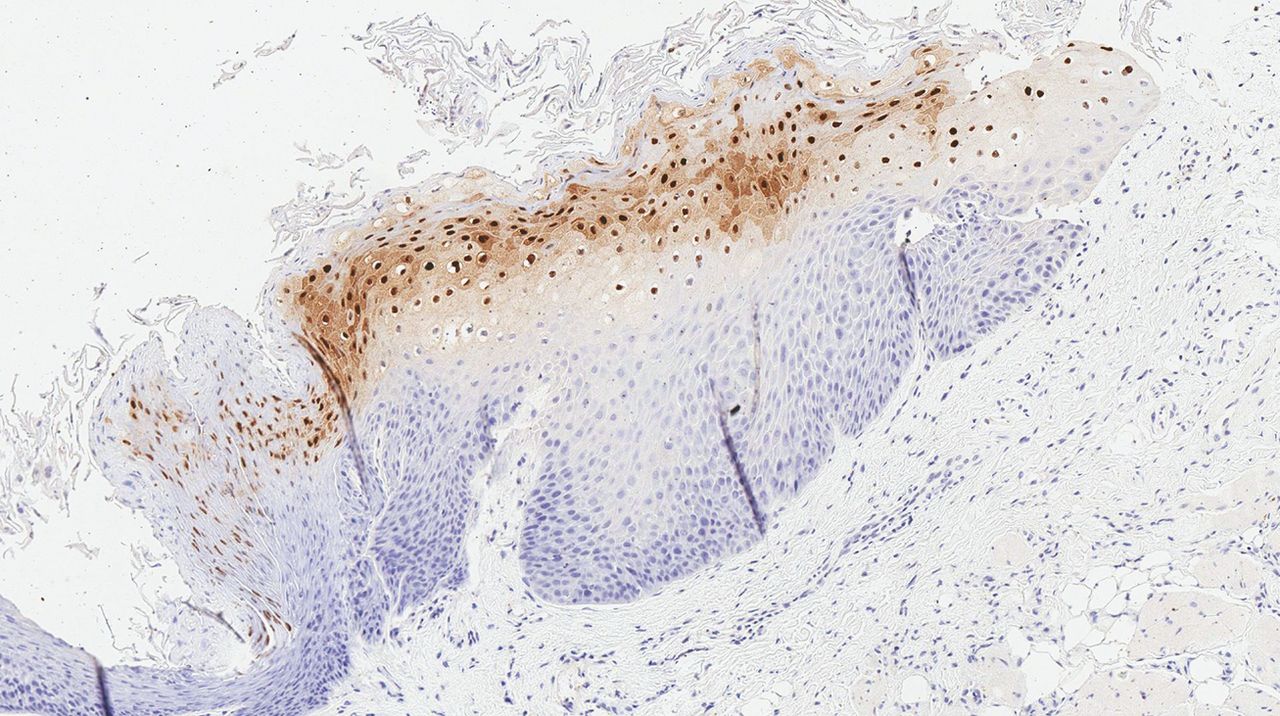
In situ hybridisation with EBER probe shows numerous positive cells in the prickle cell layer. EBER, Epstein-Barr virus-encoded RNA.
His HCL was treated with purine analogue therapy and complete morphological remission was achieved. Three months after completion of HCL treatment, the OHL lesion on the right lateral border of the tongue had resolved. He is now under the routine care of his general dental practitioner for twice yearly review. The lesion has not reoccurred.
Discussion
OHL is a benign EBV-associated lesion that most commonly presents as an asymptomatic, corrugated white patch on the lateral borders of the tongue.9 It is a well-documented phenomenon associated with immunodeficiency, but more recently has been reported in apparent immunocompetent individuals such as those using long-term inhaled steroids.7 Despite this being the first case of OHL associated with HCL in the literature, OHL has been readily described in association with other haematological malignancies. In 2010, Cho et al described a similar case of OHL presenting as the initial sign of acute myeloid leukaemia in a 15-year-old boy.19 It has also been described in individuals with multiple myeloma and acute lymphocytic leukaemia.6 20
EBV, otherwise known as human herpes virus 4, is known to infect over 95% of the world’s adult population.21 Primary infection activates the innate and adaptive immune systems, and the virus remains latent lifelong by living in memory B lymphocytes.22–24 It is primarily transmitted through saliva as infected cells are shed into the oral cavity. Despite the clearly established link between EBV and OHL, its exact role is still unclear.22 24 Debate remains as to whether OHL arises as a result of reactivation of latent strains within the tongue epithelium or as a result of repeated direct infection from EBV within the saliva.23 It has been postulated that the development of OHL occurring on the lateral borders of the tongue may be due to the resting position of the tongue in a pool of EBV-infected saliva in the floor of the mouth.23
In this case, a provisional clinical diagnosis of frictional keratosis was made due to the absence of relevant medical history. Frictional keratosis is a frequently occurring lesion that commonly presents on the lateral borders of the tongue. Certain histological features are shared with OHL, such as a corrugated hyperkeratotic surface epithelium, epithelial hyperplasia and occasional koilocyte-like cells resulting from intracellular oedema and compressed nuclei.23 Because of this, EBV detection within the lesional tissue is required for definitive diagnosis.11 However, suspicion of OHL may be raised for the reporting pathologist before the outcome of the EBER ISH due to the presence of perinuclear chromatin clumping within viral infected balloon cells.
Learning points
Oral hairy leukoplakia (OHL) is a disease entity that is no longer exclusive to patients with HIV and is now recognised as a marker of immunosuppression.
The detection of Epstein-Barr virus within the lesional tissue is required for definitive diagnosis due to shared clinical and histological features with other commonly occurring oral lesions such as frictional keratosis.
OHL does not often require treatment and will spontaneously resolve upon establishment of immune competence.
References
Footnotes
Contributors GD: literature search, drafted the manuscript and final approval of completed article. AP: contributed to the manuscript. PL: contributed histopathological information and involved in manuscript editing. KS: Evaluation and editing of manuscript to be published.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.