Article Text

Statistics from Altmetric.com
Description
A 65-year-old male, chronic smoker with chronic obstructive pulmonary disease on steroids, presented to the emergency services with decreased urine output and altered sensorium for a day. However, soon after admission, the patient sustained cardiorespiratory arrest and died. On autopsy, the lungs were heavy and consolidated with randomly distributed miliary nodules of 0.2–0.5 cm on the pleural and the cut surface of the lung parenchyma (figure 1). Perihilar, paratracheal and subcarinal lymph nodes were enlarged with caseous necrosis. Microscopically, these were composed of aggregates of macrophages along with neutrophilic infiltrates and nuclear debris (figure 2). No well-formed epithelioid cell granulomas were seen. Ziehl Neelsen stain showed numerous intracellular aggregates of acid-fast bacilli in the macrophages (figure 3). Based on histopathological features of macrophage-rich infiltrate with intracellular AFB, atypical mycobacterial infection was suspected. Multiplex PCR was performed by using IS6110 primers specific for Mycobacterium tuberculosis complex and dt6 primers specific for M. avium as described previously. The expected band size using the primers specific for M. tuberculosis and M. avium were 123 bp and 187 bp, respectively. DNA extracted from tissue samples of both lung and lymph node was positive for both M. tuberculosis and M. avium (figure 4).

Gross photograph of lung showing miliary nodules measuring 0.3 to 0.5 cm all over the cut surface of lung parenchyma.

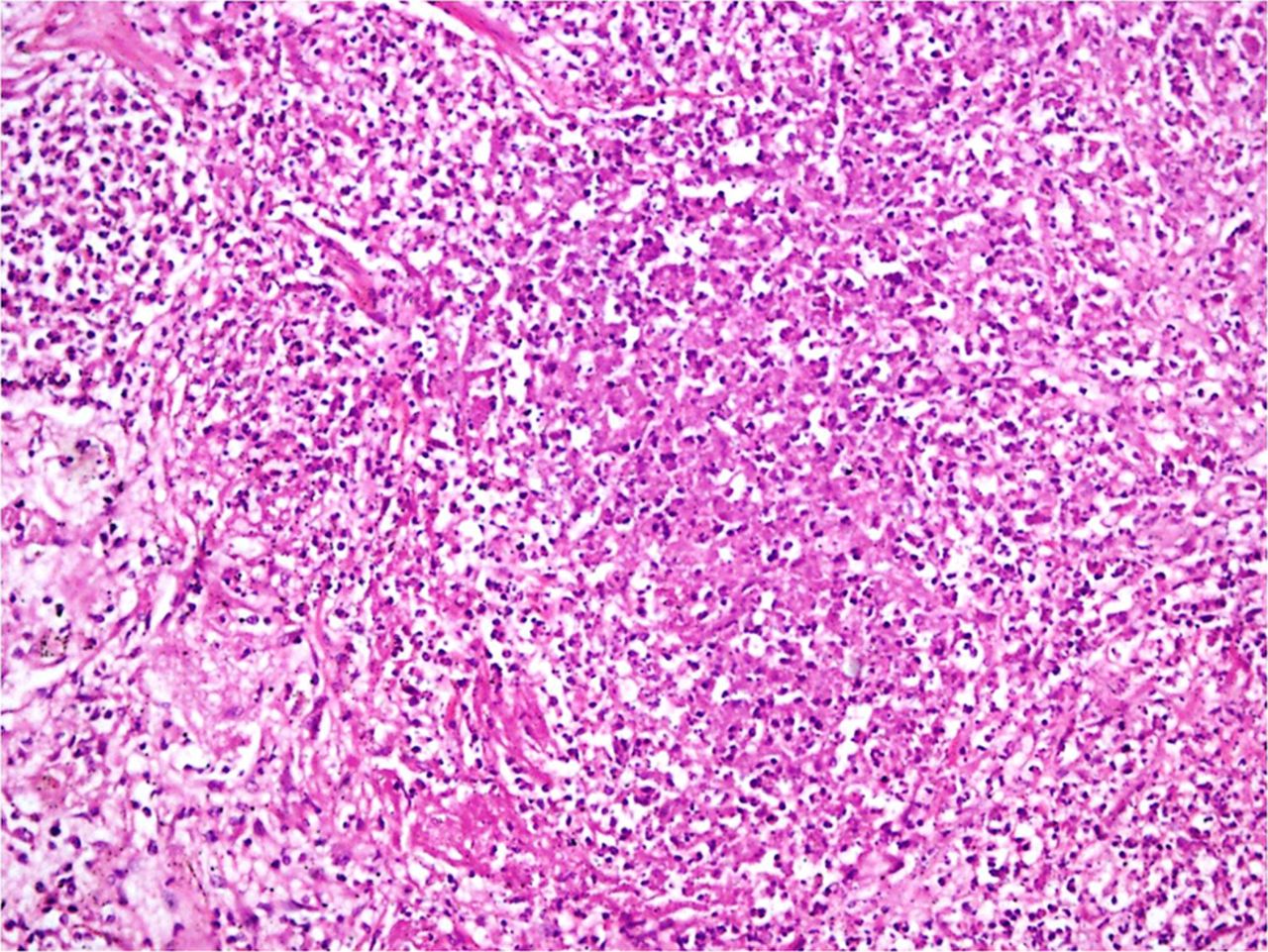
Microscopically, the nodules were composed of aggregates of macrophages along with neutrophilic infiltrates and nuclear debris. No well-formed epithelioid granulomas were seen.
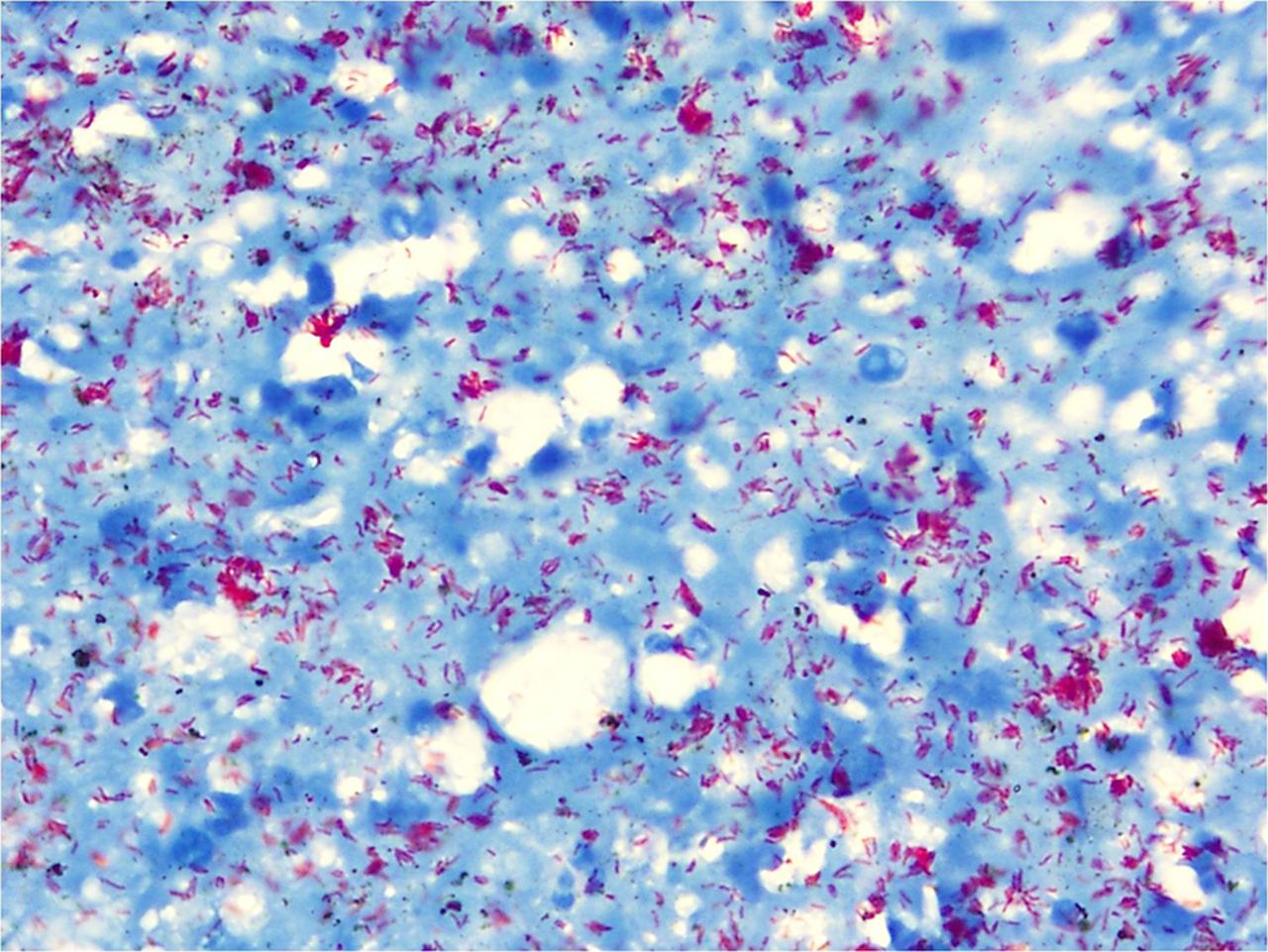
Numerous intracellular aggregates of acid-fast bacilli in the macrophages (ZN stain, ×1000).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Multiplex PCR showing specific bands for both Mycobacterium tuberculosis (123 bp) and M. avium (187 bp). L1, 100 bp mm; L2, positive control; L3, DNA from lung; L4, DNA from lymph node; L5, negative control.
Identification of both M. tuberculosis and M. avium in the same host is less quoted in literature,1–3 and the exact prevalence is not known, as most of these cases are treated as drug-resistant cases of tuberculosis. Debate exists regarding the significance of isolation of M. avium complex (MAC) from respiratory specimens, as these are ubiquitous organisms colonising the respiratory tract and are also common laboratory contaminants.3 Yet, the decisions to treat the coexistent MAC may rest on the physician, taking into account the patient’s underlying predisposing condition/immune status and responsiveness to conventional antituberculosis (TB) therapy. In an immunocompromised patient setting with failure of response to anti-TB therapy, identifying both the organisms may warrant a trial of treatment for the associated pathogen. Though treatment naive, the index case has strong histomorphological features suggesting MAC infection along with an underlying structural lung disease and a history of intake of steroids, which would possibly indicate that M. avium would rather be a coexisting offending agent and not just a coloniser.
Learning points
Clinical and histomorphological suspicion along with confirmation by ancillarytechniques like PCR is required to diagnose non-tuberculous mycobacteria (NTM) coexisting with M. tuberculosis infections. This would help in the diagnosis of coinfections due to NTM, especially M. avium and would contribute to less mortality and morbidity through appropriate treatment modalities as improvement with anti-TB drugs alone may not be seen in such patients.
Treatment of the coexisting NTM, shall be a clinical decision based on the patients pre-existing condition, immune status, histomorphological/cytomorphological clues and response to conventional anti-TB regimen.
Footnotes
Contributors Conception and design, acquisition of data or analysis and interpretation of data: PS, AB and KS. Drafting the article or revising it critically for important intellectual content: ABa and ABh. Final approval of the version published: ABa. We agree to be accountable for the article and to ensure that all questions regarding the accuracy or integrity of the article are investigated and resolved.
Competing interests None declared.
Patient consent Obtained from guardian.
Provenance and peer review Not commissioned; externally peer reviewed.