Article Text

Statistics from Altmetric.com
Description
The physiological adaptations in pregnancy can unmask underlying occult proteinuric renal disease. However, the effect of multiple pregnancies on the course of the disease is variable. We report the clinical course of a case of idiopathic membranous nephropathy through multiple pregnancies.
A 25-year-old Hispanic woman was referred to our institution for worsening generalised swelling of the body, uncontrolled hypertension and 21 g/day of proteinuria at 34 weeks' gestation during her third pregnancy. There were no stigmata suggestive of HELLP (Hemolysis, Elevated Liver enzymes, Low Platelet count) syndrome. She was previously seen at our institution 5 years ago during her 1st pregnancy when 13 g/day of proteinuria was recorded at 25 weeks of gestation. At that time, she was treated with oral steroids and delivery was induced at 35 weeks due to intrauterine growth restriction. Placental biopsy revealed focal, tightly adherent blood clot, consistent with possible abruption. Renal biopsy performed in the postpartum period was consistent with membranous nephropathy (figure 1).

Renal biopsy consistent with membranous nephropathy (A) H&E section showing thickened capillary loops (arrows); (B) silver stain showing thickened basement membranes (arrows); (C) immunofluorescence for IgG showing fine granular positivity; and (D) electron microscopy showing subepithelial deposits (arrows).
She was treated with ACE inhibitors (ACEI) and at 3-month follow-up, she was asymptomatic, without oedema and urine protein–creatinine ratio (UPCR) had decreased to 7 g/g. She was lost to follow-up for 5 years until this recent admission. In the interim, she apparently had a second successful pregnancy but no data was available. During current pregnancy, delivery was induced at 34 weeks and the placental biopsy showed that it was critically small for gestational age and had focal intervillous fibrin deposition together with focal calcifications in the areas of more significant ischaemia (figure 2). Serology for antinuclear antibody, anti-double-stranded DNA, antiphospholipid antibody, viral hepatitis and rapid plasma regain were negative. Serum complements were within normal limits. During both the pregnancies, she had hypertension with average blood pressures in the range of 140–150/80–90 mm Hg, which is higher than expected for a normal pregnancy but within acceptable range for patients with pre-existing chronic hypertension. At 1-month post-partum, UPCR was 1.8 g/g, without any treatment. Interestingly, her serum creatinine ranged between 0.6 and 0.9 mg/dL during this 5-year period. The patient was once again lost to follow-up.
{kind=link}
{kind=link}
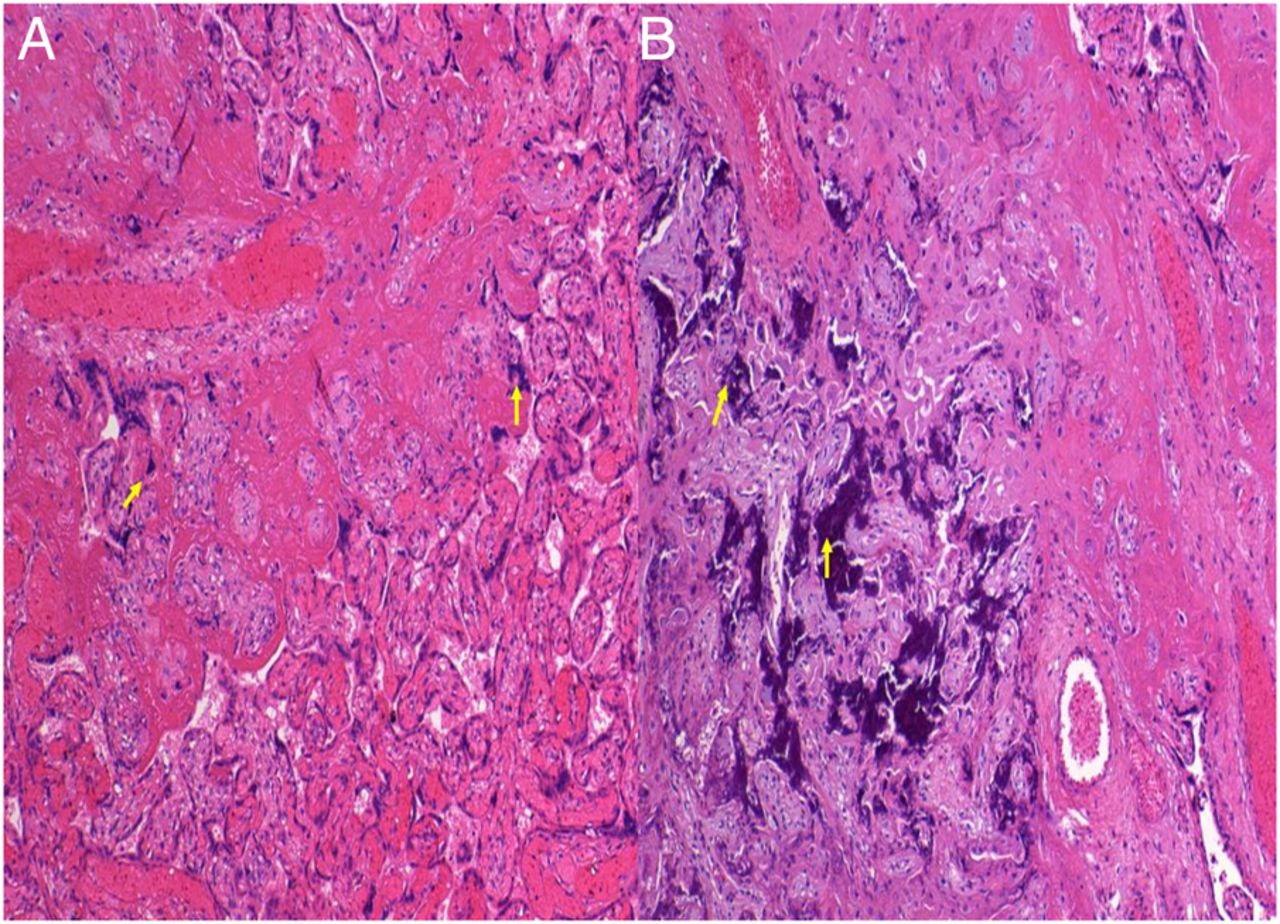
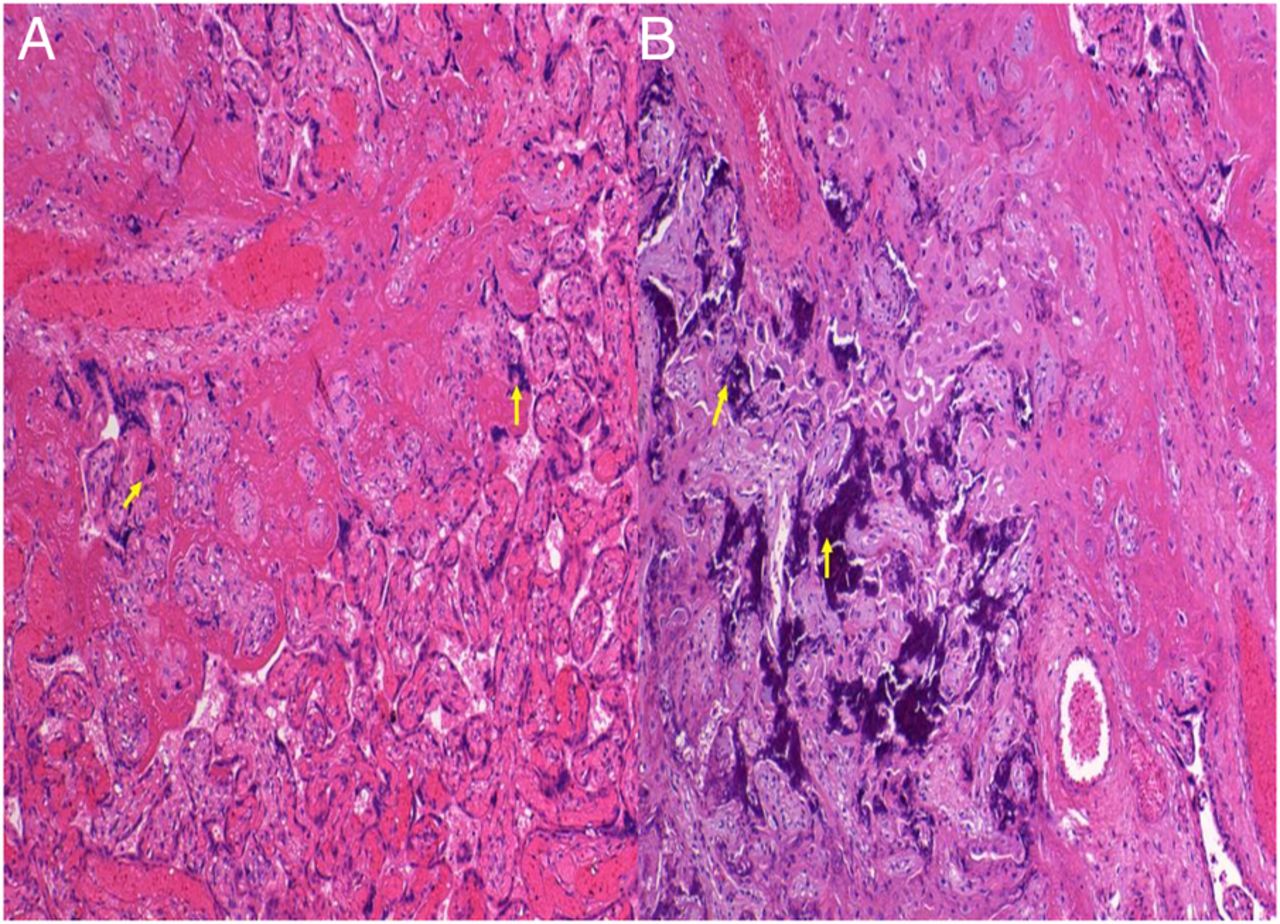
Placental biopsy showing (A) focal intervillous fibrin deposition (arrows) and (B) focal calcifications (arrows) in the areas of significant ischaemia.
Learning points
Although there is physiological increase in proteinuria during pregnancy, the presence of nephrotic range proteinuria with or without hypertension in any trimester is always pathological and may be associated with underlying renal disease and a poor prognosis.1
Our case supports that spontaneous remission of membranous nephropathy can occur despite physiological changes associated with pregnancy and the natural course of the disease probably follows that of non-pregnant individuals.
Pregnant patients with high-grade proteinuria are at increased risk for placentofetal complications including intrauterine growth restriction, preterm delivery and fetal demise as evidenced by our case and existing literature.2 ,3 Also, our patient had hypertension, which is an independent risk factor for such complications.
Footnotes
Contributors AK and AV have prepared the initial draft. DNW has procured the images and AAE has critically revised the manuscript for important intellectual content. All the authors approved the manuscript for final submission.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.