Article Text

Statistics from Altmetric.com
Description
A 50-year-old woman with no cardiovascular risk factors was evaluated for easy fatigability and progressive dyspnoea on exertion for the last 1 year. Cardiac auscultation revealed a normal first heart sound, an ejection systolic murmur at the upper left sternal border and wide and fixed splitting of the second heart sound. The ECG demonstrated sinus rhythm, incomplete right bundle branch block (RBBB) and ‘crochetage’ sign (notch near the apex of the R wave) in inferior limb leads (figure 1). There was evidence of cardiomegaly, dilated main pulmonary artery and pulmonary plethora on the chest X-ray. Atrial septal defect (ASD) was suspected and two-dimensional transthoracic echocardiography (TTE) subsequently confirmed the presence of a large ostium secundum ASD with right ventricular volume overload. There was mild tricuspid regurgitation and the estimated right ventricular systolic pressure was 38 mm Hg. Transoesophageal echocardiography established the presence of an 18 mm ostium secundum ASD with adequate margins and normal pulmonary venous drainage. The calculated Qp/Qs was 3.0 on cardiac catheterisation study. Coronary angiography displayed normal epicardial coronary arteries. She underwent successful device closure using a size 24 mm Cocoon Septal Occluder (Vascular Innovations Co., Thailand). Two months after the procedure, the ECG showed disappearance of crochetage on R wave with persistent incomplete RBBB pattern. The TTE revealed the device in situ and no evidence of any residual shunt or right ventricular volume overload.
{kind=link}
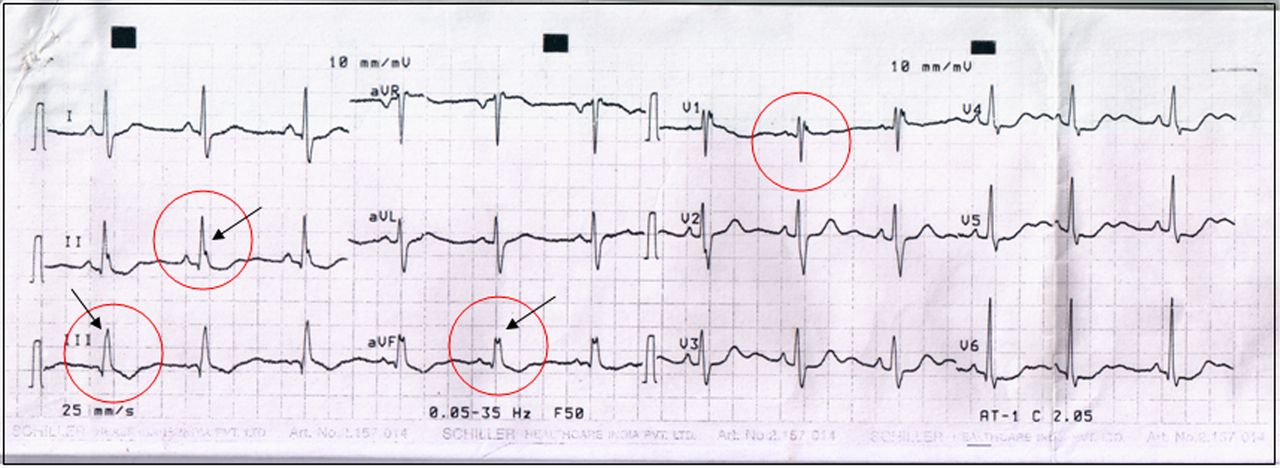
ECG of a 50-year-old woman with a non-restrictive secundum atrial septal defect and a 3.0–1 left-to-right shunt. Crochetage is represented by notches on the R waves (arrow and circle) in leads II, III, and aVF. There is incomplete right bundle branch block pattern in lead V1 (circle).
Crochetage is independent of the incomplete RBBB pattern, but when RBBB occurs with crochetage in all inferior limb leads, as in this index case, the specificity of the ECG diagnosis of ASD is remarkably high.1 Although crochetage has been correlated with shunt severity, the pattern has been reported with a patent foramen ovale (PFO) and has been suggested as an ECG marker of a PFO associated with ischaemic embolic stroke.2
Learning points
A notch near the apex of the R wave in inferior limb leads of ostium secundum atrial septal defects has been called ‘crochetage’ because the notch resembles the work of a crochet needle.1
Its incidence increases with larger anatomical defect or greater left-to-right shunt even in the presence of pulmonary hypertension.1
Early disappearance of this pattern was observed in 35.1% of the operated-on patients although the right bundle branch block pattern persisted.1
Footnotes
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.