Article Text

Statistics from Altmetric.com
Description
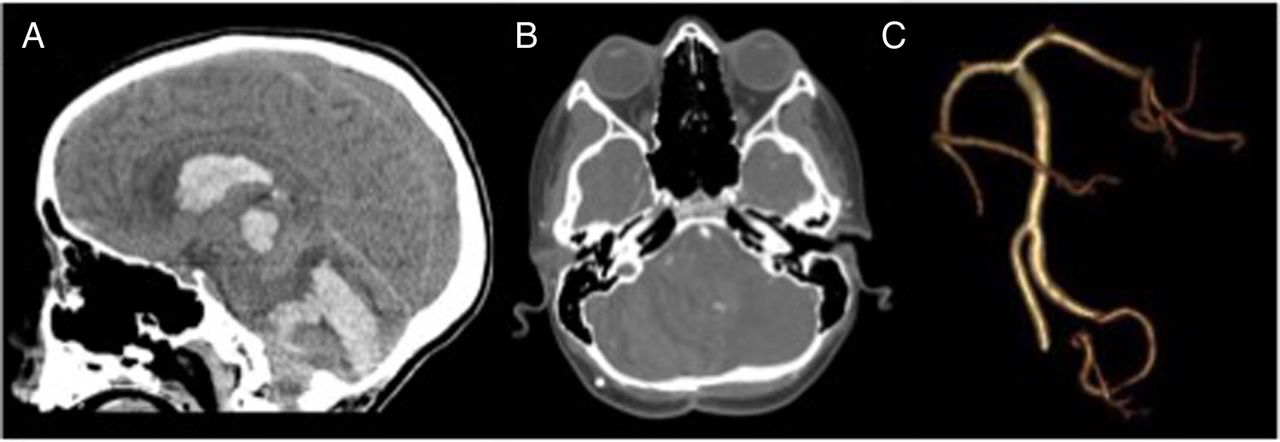
A 9-year-old boy with a history of posterior fossa juvenile pilocytic astrocytoma presented to the emergency room for lethargy and worsening headache. Three years earlier, he underwent near total resection of the tumour. Owing to the progressive disease, he had a second resection and underwent conformal radiation therapy, totalling 5040 cGy. In the following 2 years, he reported of severe headaches. Multiple brain MRIs with and without contrast and head CTs without contrast did not reveal disease recurrence or significant abnormality. On the day of presentation, the child again reported of a severe headache and was brought to the emergency department (ED). In the ED, he rapidly decompensated. Neurological examination showed a large and non-reactive right pupil. CT of the head revealed a spontaneous fresh haemorrhage in the right cerebellum. CT angiography showed an abnormal tangle of vessels off the right posterior–inferior cerebellar artery (figure 1A–C). Neurosurgical intervention confirmed the presence of an aneurysm. The child died 13 days after the presentation.

{kind=link}
CT head angiography. (A) Large posterior fossa haemorrhage with extension into the ventricular system. (B) Demonstration and (C) three-dimensional reconstruction of prominent tonsillar branch arising from the PICA with a small abnormal irregular vessel, likely a small aneurysm.
Radiotherapy is a part of the standard treatment for many paediatric brain tumours. It is, however, not without risk. Cranial irradiation can cause a multitude of problems including stroke, neuroendocrine abnormality, cognitive deficit and vascular malformations.1 Children who report of severe headaches postcranial radiation have a greater risk of neurovascular events.2 While vascular complications after cranial radiotherapy are well documented, aneurysm is rare. A retrospective chart review study published in 2006 showed that 3% of the 224 paediatric patients who received cranial radiotherapy developed aneurysm and one developed a rupture aneurysm.3 However, although rare, recurrent headaches in a patient with prior radiation therapy should raise suspicion of aneurysm even in the presence of normal MRI. Therefore, CT or conventional angiography may be considered.
Learning points
Cranial irradiation, while it can be a part of standard therapy for paediatric brain tumour, is not without its risk, and has been shown to cause a number of problems, including vascular malformations.
Consider CT or conventional angiography to rule out aneurysm for patients with headache with history of cranial irradiation.
Footnotes
Contributors JRC and MLL were involved in diagnosis and treatment of the patient. DYC and JRC did the literature search and wrote the manuscript. JRC is responsible for the overall content as the guarantor.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.