Article Text

Statistics from Altmetric.com
Description
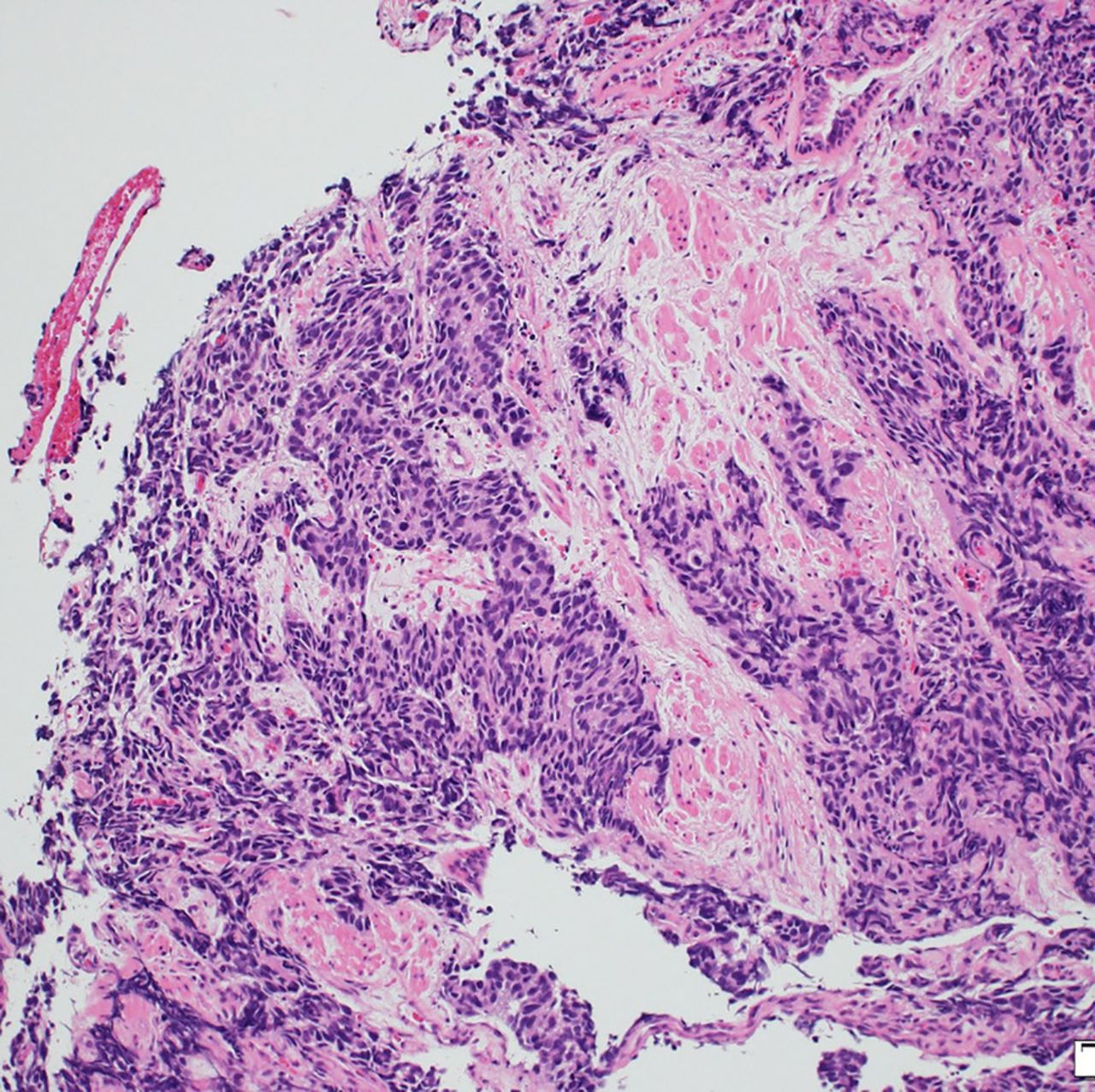
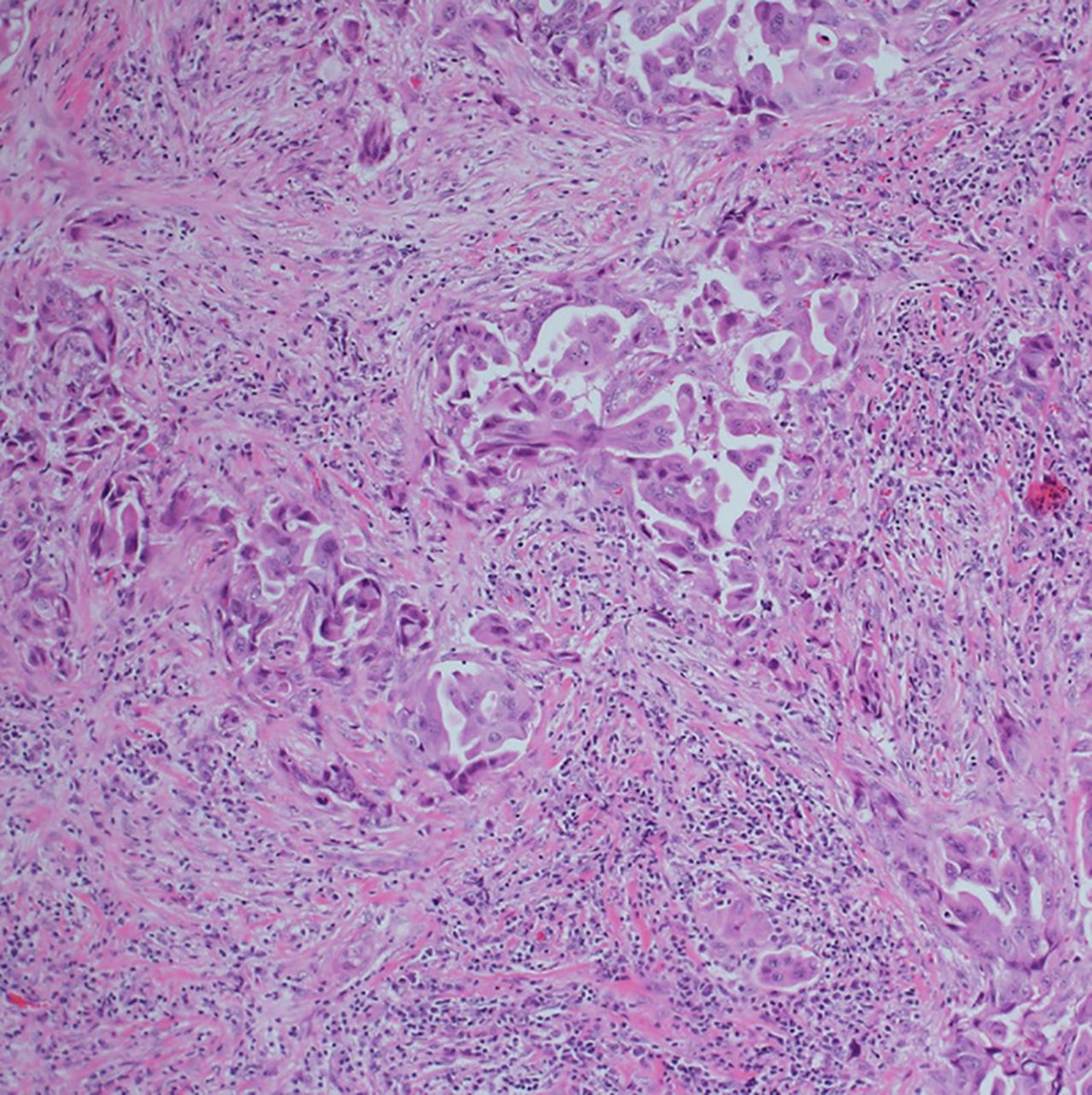
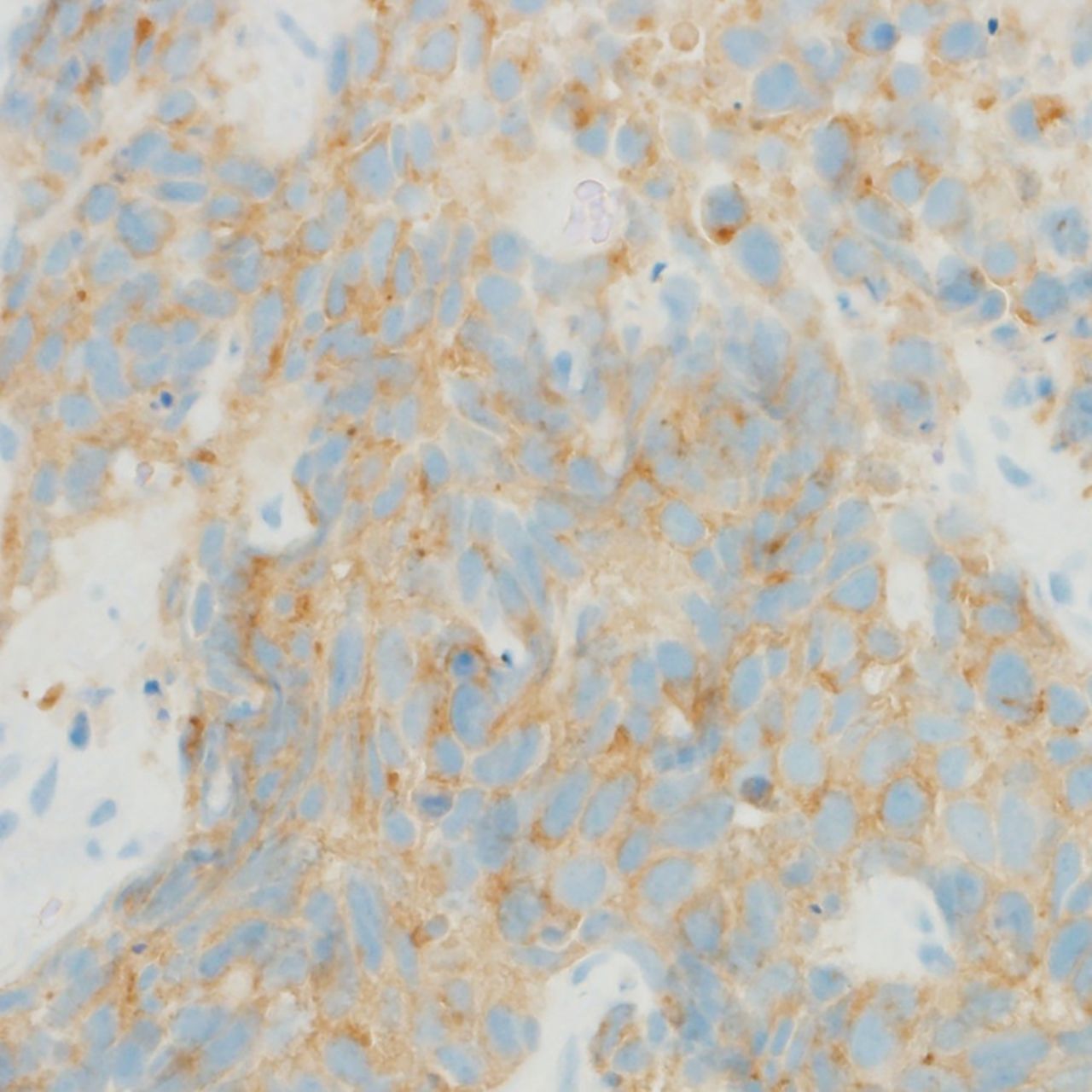
A 58-year-old woman with no history of smoking was admitted to our hospital with exacerbation of cough. CT of the chest revealed a left upper lobe lung tumour. Bronchoscopic biopsy of the tumour revealed stage IV poorly differentiated adenocarcinoma (figure 1) with epidermal growth factor receptor (EGFR) gene mutation (L858R point mutation). After cytotoxic chemotherapy (cisplatin and pemetrexed) as first-line therapy, disease progression was identified. For the next 3 years, she was treated with erlotinib, an EGFR tyrosine kinase inhibitor (TKI). Regimens were changed several times (cisplatin, gemcitabine, docetaxel and afatinib) due to disease progression or adverse effects. After 2 months with afatinib, disease progression was again noted. We once again performed bronchoscopic biopsy of the primary tumour, and small cell lung cancer (SCLC) was confirmed from histopathological examination (figures 2⇓–4). Levels of tumour markers such as progastrin-releasing peptide and non-specific elastase were elevated. Moreover, a second examination again detected the EGFR gene mutation (L858R point mutation without T790M point mutation). Amrubicin was administered, resulting in radiologically stable disease. Most cases of acquired resistance to EGFR-TKI arise from the emergence of T790M mutation, and morphological transformation to SCLC is rare.1 After the failure of EGFR-TKI, rebiopsy of the tumour is warranted to determine the next treatment strategy.

H&E staining.
H&E staining.

Chromogranin A staining.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Synaptophysin staining.
Learning points
After the failure of epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKI), rebiopsy of the tumour should be performed to determine the next treatment strategy.
But it is unclear when to perform rebiopsy after EGFR-TKI failure.
Reference
Footnotes
Contributors YH, JN and NN participated in patient care. YH wrote the manuscript and YK revised it.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.