Article Text

Statistics from Altmetric.com
Description
A 46-year-old man, an engineer, presented with chronic left calf pain and tingling sensation in the foot for the past 2 years. There was no history of associated back pain and spine MRI study (performed elsewhere) was essentially normal. Several medics had treated the patient conservatively, yet his symptoms persisted. At the time of presentation, he also pointed out a slow growing swelling in the left popliteal fossa, of 3 months’ duration. Clinical examination revealed a small, mobile, non-pulsatile, non-transilluminant, non-tender soft tissue swelling in the popliteal fossa.
Ultrasonography of the popliteal fossa observed a well-defined heterogeneous mass suggestive of a Baker's cyst. In prone position, the popliteal fossa was exposed through a lazy S incision. A firm nodular encapsulated swelling was dissected and found to be adherent to the tibia nerve. Excision was accomplished without dividing the tibia nerve (figure 1). The diagnosis of ancient schwannoma was established by histopathological assessment (figure 2). The patient did not exhibit any neurological deficits in the postoperative period and, at 23 months of follow-up, is symptom-free.

Intraoperative photograph of a schwannoma of the tibia nerve (black arrow) in the popliteal fossa (inset: gross specimen of the excised tumour (nodular and greyish-white)).

{kind=link}
{kind=link}
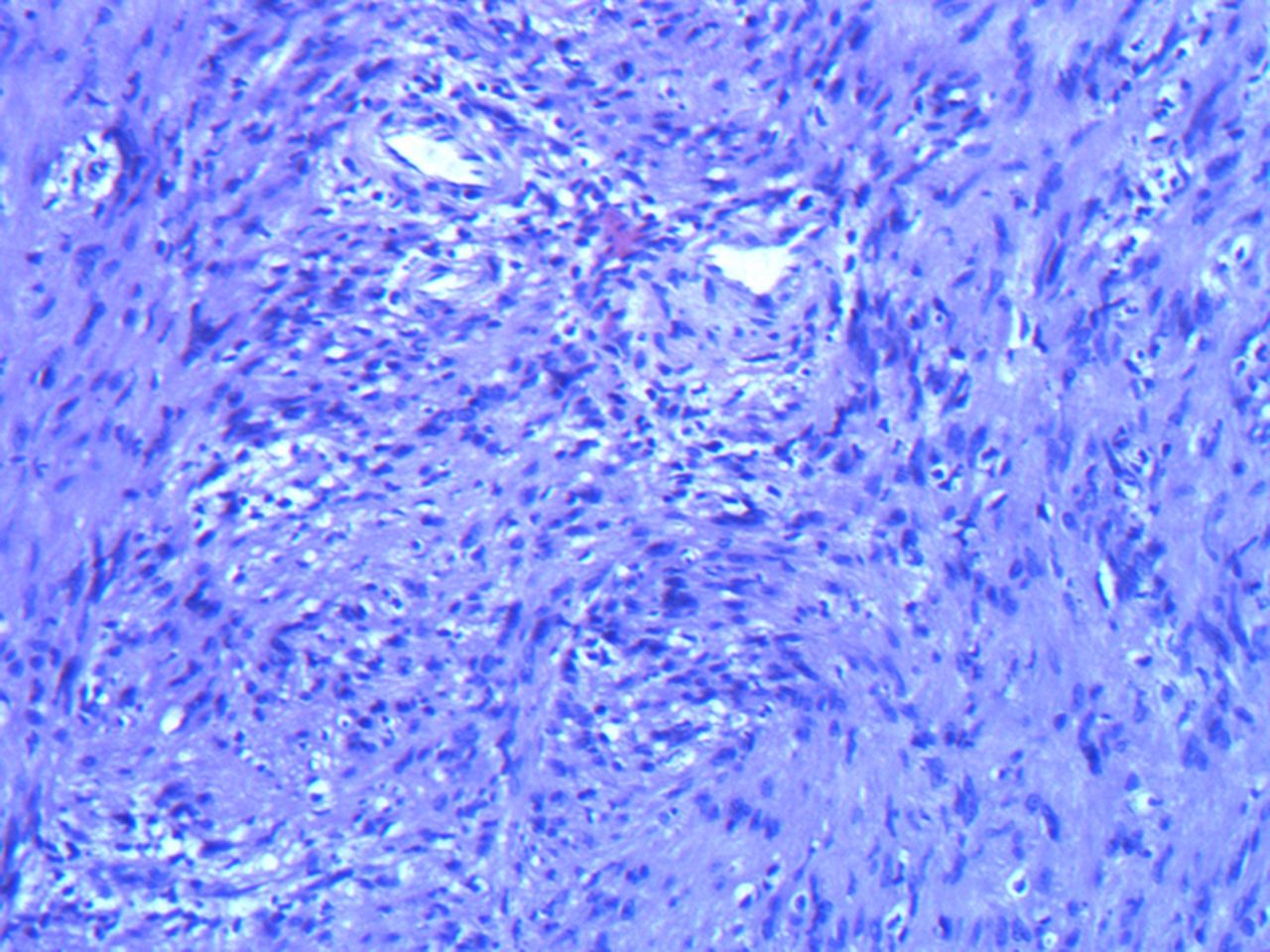
Spindle cells with eosinophilic cytoplasmic processes and palisading forming Verocay bodies. Also seen are congested vessels with perivascular hyalinisation, stromal hyalinisation, haemorrhage and hemosiderin and fibrin deposition (×10; H&E stain).
Discussion
Schwannomas are slow growing painless benign peripheral nerve sheath tumours that are rarely seen to occur in the lower limbs. Clinical presentation is often misleading and ambiguous. The schwannoma of a tibial or sciatic nerve may cause radicular leg pain, which leads to a diagnosis of lumbosacral radiculopathy, chronic regional pain syndrome, tarsal tunnel syndrome, entrapment neuropathies or diabetic neuropathy.1 The diagnosis in the index case was overlooked as sonographic evaluation suspected it to be a Baker's cyst—the most common popliteal swelling—which can occasionally produce compression neuropathy of the tibial nerve.
On sonography, schwannomas appear as well-defined, ovoid, heterogeneous masses in conjunction with cystic degeneration, eccentric location and posterior acoustic enhancement.2 MRI is another preferred tool that can define the nerve–tumour relationship. The lesion presents as a well-defined mass, usually fusiform in shape, located within the nerve, isointense to surrounding muscles on T1-weighted images and hyperintense on T2-weighted images.3 Ultrasonography, CT and MRI are all useful modalities in the preoperative diagnostic work up of this nerve tumour, however, each of these imaging studies has limitations in distinguishing between the different types of nerve sheath tumours aside from problems differentiating between benign and malignant lesions. Sometimes, long-standing slow growing nerve tumours are known to exhibit degenerative features as seen in the index case. The term ‘ancient schwannoma’ is used to describe such a rare subset, which can occasionally be misinterpreted as sarcomatous changes. Surgical excision ensures prompt symptomatic relief with a favourable prognosis.
Learning points
Tibial nerve schwannoma is a rare popliteal fossa swelling with obscure clinical presentation.
The diagnosis of tibial nerve schwannoma is often established late as it can be mistaken for a radiculopathy or, infrequently, a Baker's cyst producing compression neuropathy.
On sonography study, based on certain imaging features, this lesion can be reasonably identified or provide a differential diagnosis, however, it can easily be overlooked by the unsuspecting radiologist as well as by clinicians, which can result in intraoperative surprises.
Footnotes
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.