Article Text

Summary
Plasma cell neoplasms (plasmacytoma) are discrete, solitary masses of lymphoid neoplastic proliferations of B cells. Plasmacytomas comprise three groups: multiple myeloma, solitary plasmacytoma (SP) and extramedullary plasmacytoma. SP originates as a clone of transformed malignant plasma cells in the bone marrow. SP of the jaw is a rare condition; therefore diagnosis is quite difficult and often results in misdiagnosis. MM is a lymphoproliferative disease the prognosis of which is worse than SP. SP can progress to MM in a few months to years after diagnosis. In this regard, early diagnosis of the disease is of utmost importance. This article presents two cases of SP diagnosed in the mandible and documented with clinical, radiographic and histological findings.
Statistics from Altmetric.com
Background
Plasma cell neoplasms (plasmacytoma) are discrete, solitary masses of lymphoid neoplastic proliferations of B cells.1 The incidence of plasmacytoma is about 2.6–3.3 per 100 000 population. The average age of presentation is after 50s. Plasmacytomas are most commonly found in long bones and the backbone. They rarely occur in the jaw. Plasmacytomas comprise three groups: multiple myeloma (MM), solitary plasmacytoma (SP) and extramedullary plasmacytoma (EMP). SP occurs centrally localised in bones and EMP in soft tissues; while MM is a multifocal disseminated form of plasmacytomas.2
Case presentation
Case report I
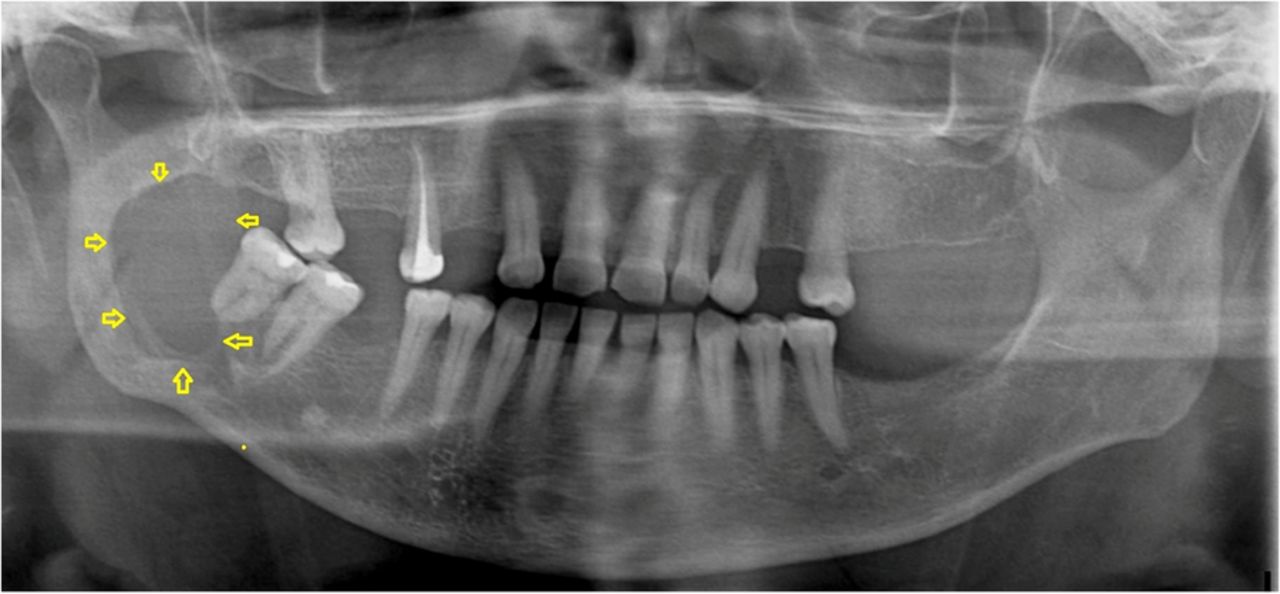
A 67-year-old woman was admitted to our department, with pain in the right mandibular ramus region. She had moderate paraesthesia on the related side. Orthopantomography revealed a unilocular radiolucent lesion extending from the mandibular ramus to the second molar tooth. The lesion was approximately 25×30 mm in dimension and was covered with intact mucosa (figures 1 and 2). Incisional biopsy was performed. During the surgical procedure, excessive bleeding was observed, which continued for more than 5 h despite preventative applications.
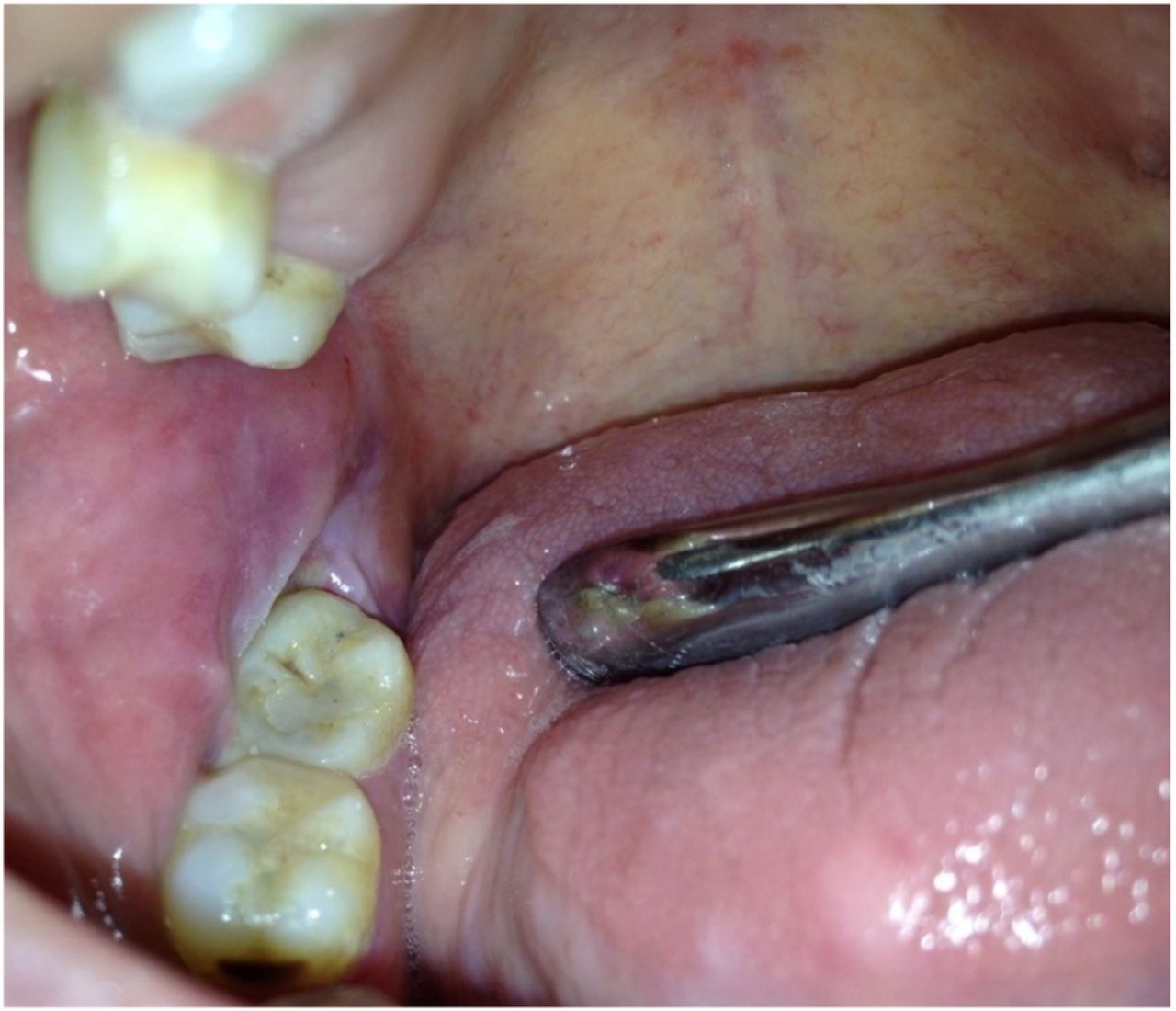
Intraoral appearance of the first case.

Orthopantomography of the first case.
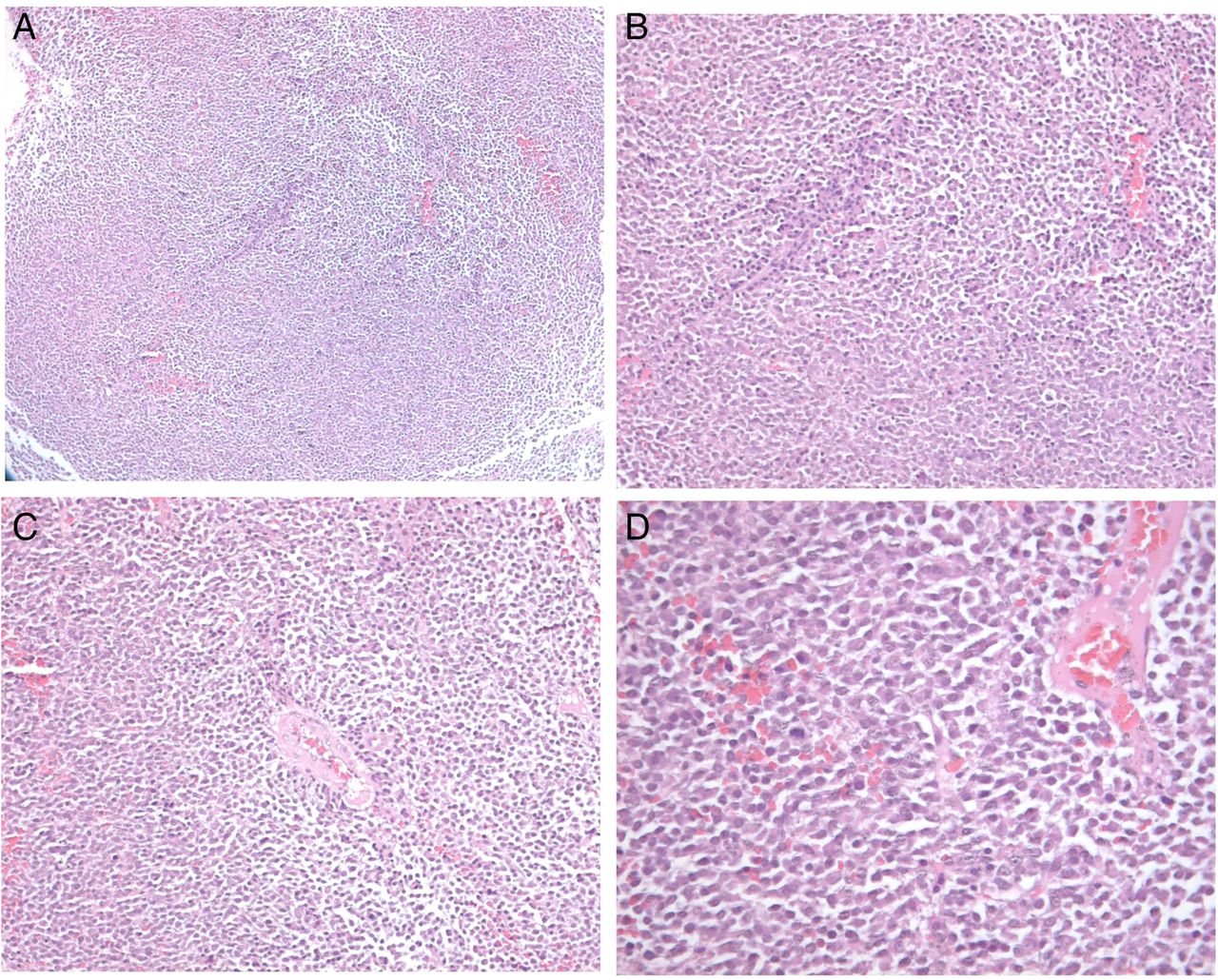
The histopathological examination revealed a sheet-like growth pattern of tumoural lesion composed of malignant plasma cells. The plasma cells were pleomorphic, and had significant and hyperchromatic nuclei with eosinophilic cytoplasm (figure 3). Tumour cells were found to be monoclonal by immunohistochemical staining of κ and λ. The λ-light-chain level was detected to be as high as 1940 mg/L. In biochemical analysis, the β-2 microglobulin level was noted as 3.13 mg/L. The diagnosis of SP was made.

Histopathological images of the first case (A) Sheet-like pattern of atypical plasma cells, H&E staining, magnification of ×200. (B) Plasma cells stained positive for λ light chains. (C) Demonstrating monoclonality of the tumour and cells were negative for κ light chains.
The patient was referred to the oncology department for further investigations and treatment. The final diagnosis was MM. Unfortunately, the patient died before the treatment was finished.
Case report II
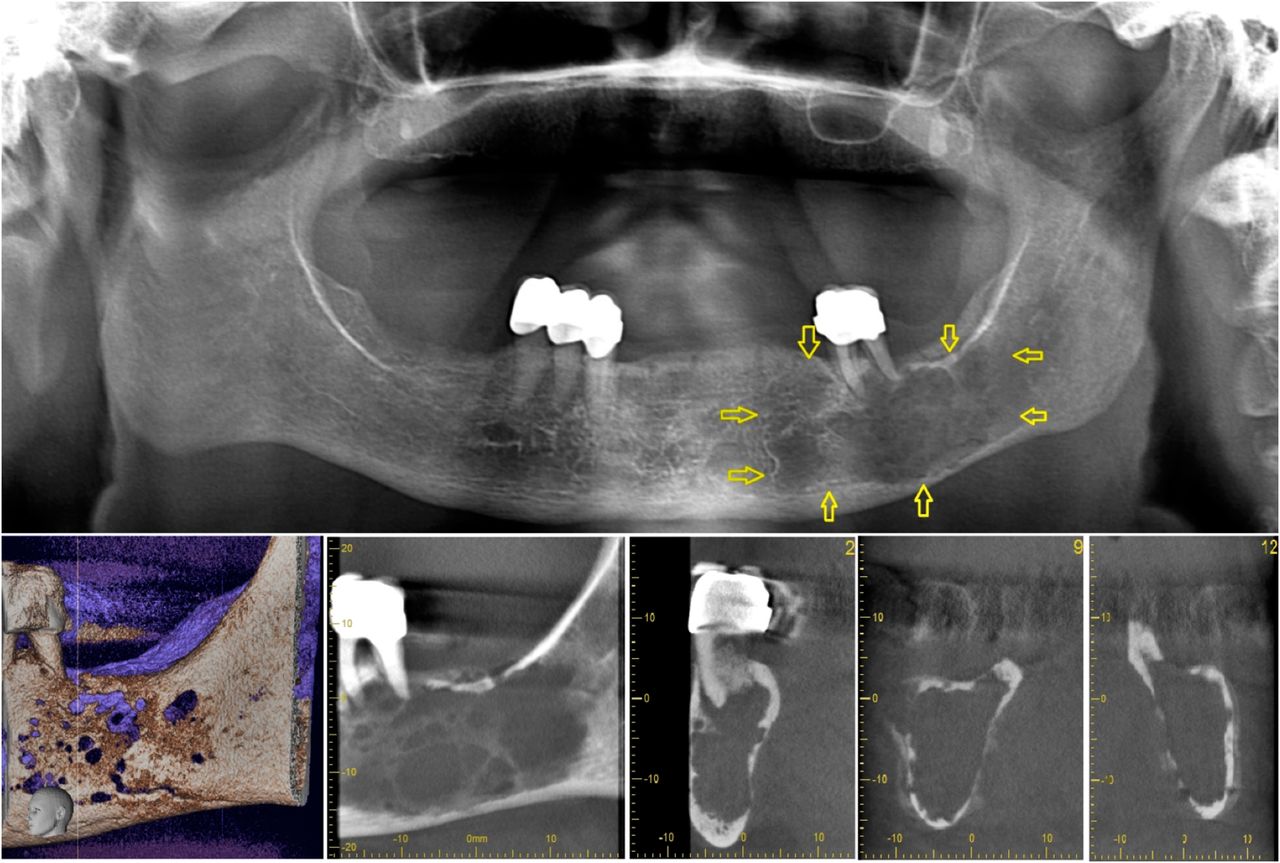
A 61-year-old woman was admitted to our department, with the primary symptom of mild pain in her left mandible. She also reported of numbness in her left lip and chin. The lymph nodes were not palpable. The patient's medical history was unremarkable and physical examination revealed no other abnormality. Orthopantomography and cone beam CT revealed the presence of an ill-defined, multilocular radiolucent lesion extending from the first premolar region to the angle of the mandible (figure 4). The lesion was covered by normally appearing mucosa.

Orthopantomography and cone beam CT images of the second case.
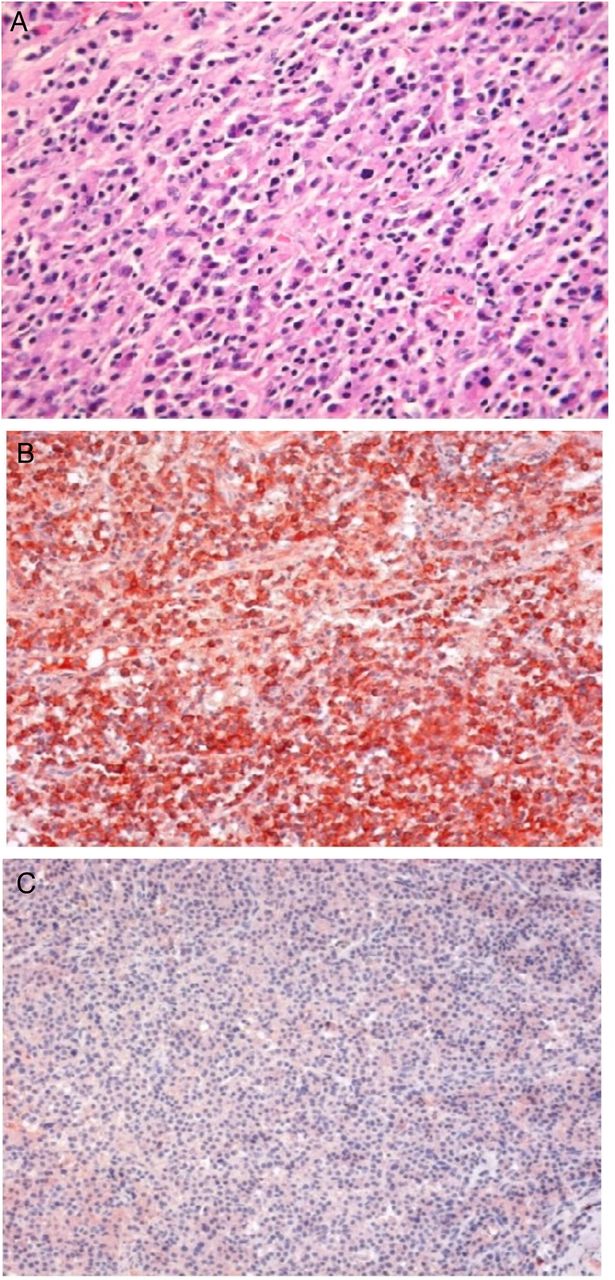
Aspiration biopsy was non-productive, thus excluding the possibility of vascular or cystic lesions. An incisional biopsy was performed under local anaesthesia, during which profuse intraoral bleeding was noted. Histopathological examination of the specimen revealed atypical plasma cells with large hyperchromatic nuclei (figure 5). The histopathological examination was suggestive of SP.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Histopathological images of the second case, H&E staining showing sheets of tumour cells resembling plasma cells (A:10×, B:20×, C:20×, D:40×).
The patient was referred to the oncology department for further investigations. The diagnosis of MM was made as the patient had M-protein in serum and urine, and a high level of bone marrow plasma cells on tissue biopsy. Also, further radiological examination showed multiple punched-out radiolucent lesions in the skull and pelvis, which led to a radiological diagnosis of MM.
Differential diagnosis
The differential diagnosis of radiolucent lesions that show improvement similar to plasmacytomas in the posterior mandible may be ameloblastoma, odontogenic myxoma, central giant cell granuloma and odontogenic keratocyst.3 ,4
Although a soap bubble appearance was not exactly detected in our cases, the locations of the lesions and especially the multilocular structure of our second case, led to a doubt for ameloblastoma. However, as our patients were over 60 years, ameloblastoma was not primarily considered for an initial diagnosis.
As a typical finding of odontogenic myxomas the paper thin trabeculae were not seen in the radiograph of the our cases, but the aggressive behavior leading to bony expansion and the irregular radiographic outline hinted toward to odontogenic myxomas.
In our cases, aggressive structures of central giant-cell granulomas were evaluated for initial diagnosis due to their multilocular radiological appearances and their growth by widening towards the buccolingual direction. Despite this, our patients being old did not comply with diagnosis.
In our first case, while radiographic findings made us consider unilocular keratocysts, in the second case, unclear bounded multilocular fields were not matching up with keratocyst findings. Besides, in both cases, the aspiration biopsies gave negative results.
Plasma cell infiltrations may also be seen in various odontogenic infections, and, when diagnosing, they should be distinguished from plasmacytoma. While most of the inflammations that show a high plasma cell infiltration include other leukocytes and, especially, collagen stroma, in plasmacytomas, the cells are in homogenous form. Furthermore, in inflammations, plasma cells are of a polyclonal form and thus in immunohistochemistry results, they would indicate both κ and λ light chain. Plasmacytomas, on the contrary, are of a monoclonal form and they would indicate only one of either κ or λ light chain.5 In our cases, monoclonal and cytoplasmic reaction is positive only for λ light chain in the immunohistochemistry. This situation distinguishes our cases from inflammations.
Discussion
SP of the jaws is a rare condition; therefore diagnosis is quite difficult and often results in misdiagnosis.6 It is reported that plasmacytomas are seen in the nasal cavity and sinus in 40% of cases, in the nasopharynx in 20% and in the oropharynx in 18% of cases, within the maxillofacial region.5 The rate of incidence of plasmacytoma on the mandible has been reported as 4.4%. They are most frequently seen in the posterior and ramus of the mandible, which are bone marrow-rich regions.7 Pisano et al8 reported that, in 9 of 13 cases, lesions were on the posterior part of the premolars and in only one case was the lesion in the anterior region. Also, Lae et al9 reported that, in 15 of 21 cases, lesions were observed in the maxilla and only 6 were in the mandibular. In our cases, both lesions were seen in women, and these lesions were in the posterior region of the mandible.
The oral symptoms of plasmacytomas usually occur as pain, tooth ache and mobilisation, paraesthesia, swelling and pathological fractures.1 ,5 In our cases, both patients had pain and paraesthesia.
The prognosis of the disease and the survival rates of the patients vary depending on the differentiation of the plasmacytomas. There are three different groups according to their dysplasia: dysplasia at low level (plasmablastos lower than 10%), dysplasia at middle level (plasmablastos between 10% and 50%) and severe dysplasia having the worst prognosis with more than 50% in an immature form.2 Our cases may be classified as middle level, as approximately 40% dysplasia was seen.
SP may be an isolated disease or the first manifestation of a subsequent MM. Zachriades et al10 reported that plasmacytoma of the jaws may be an indication of MM, with an advancement rate of 65–100% in 15 years. The isolated form of plasmacytoma seems to have a better prognosis, while in cases of subsequent MM, the prognosis may be different. An et al11 reported that 5-year survival rate of SP is 60%; however, it goes down to 5.7% when progression to MM occurs.
Plasmacytomas generally respond positively to radiotherapy. Local radiation and chemotherapy may defer MM transformation. Some authorities suggest radiotherapy following surgical excision for the treatment of SP.4 In our cases, the patients were referred to the oncology department for treatment but, unfortunately, one of our patients died before the treatment was finished.
Learning points
Solitary plasmacytoma (SP) of the jaw is a rare condition, especially in the mandible; therefore diagnosis is quite difficult and often results in misdiagnosis.
Simple diagnostics tools such as orthopantomography are valuable for initial diagnosis. The differential diagnosis of plasmacytomas in the posterior mandible may be ameloblastoma, odontogenic myxoma, central giant cell granuloma and odontogenic keratocyst.
SP can progress to multiple myeloma (MM), the prognosis of which is worse than SP. Therefore, early diagnosis of the disease is very important. For the dentist, oral manifestations of SP or MM should be taken into consideration.
Footnotes
Contributors SKu and NBK were responsible for treatment of the patient. SKu and BK followed-up the patient. SKu, NBK and SKa were responsible for preparation of the manuscript. BS conducted pathological evaluation. SKa was responsible for critical revision of the manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.