Article Text

Statistics from Altmetric.com
Description
A 46-year-old woman presented with a large painless mass, present for over 10 years, on her right mid-lower back. However, it had increased in size over the past 3 years.
She was a heavy-smoker, with a history of chronic obstructive airway disease.
On examination, there was a large pedunculated mass located on her right mid-lower back (figure 1A–C, lateral view; figure 1D, E, close-up view). It was firm to the touch and non-tender. She had no other skin lesion and there were no palpable nodes. The rest of the examination was normal.

Photographs showing a large pedunculated mass measuring 19×17 cm (A–C, lateral view; D and E, closer view).
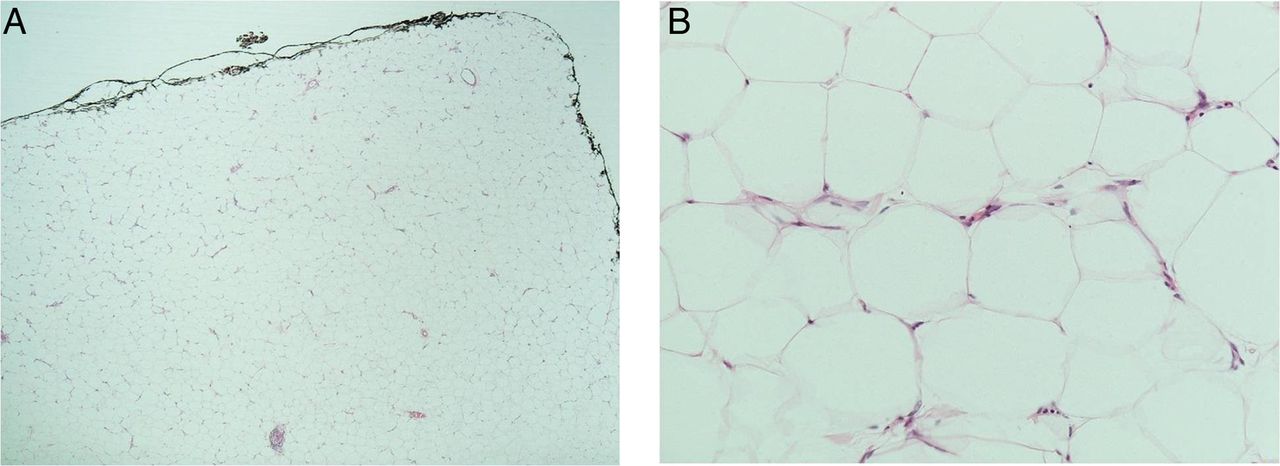
Given the clinical findings, an MRI was performed due to concern for an underlying sarcoma (figure 2A, B, MRI-sagittal view; figure 2C, MRI axial view) reported a 19×17×6.7 cm (Craniocaudal × transverse × AP) mass at mid-thoracic to upper lumbar area. It demonstrated uniformly high T1 and T2 signals and was suppressed on the T1 fat-suppressed sequence. There was no abnormal enhancement and no communication between the mass and the underlying spine. Histology (figure 3A, low power; figure 3B, high power) reported findings consistent with a lipoma.

MRI reported a 19×17×6.7 cm (craniocaudal × transverse × AP) mass extending from mid-thoracic to upper lumbar levels. It demonstrated uniformly high T1 and T2 signal and was suppressed on the T1 fat-suppressed sequence. There was no abnormal enhancement and no communication between the mass and the underlying spine (A, sagittal view; B, close sagittal view; C, axial view).
{kind=link}
{kind=link}
{kind=link}
Histology—sheets of mature adipose tissue in keeping with a benign lipoma (A, low power; B, high power).
Lipomas are benign neoplasms made up of adipocytes. They can occur on any part of the body but frequently occur in the trunk and upper extremities. They are likely to present in the 40–60-year age group.1 They are usually painless, soft and small, at about 1 cm, but can be giant lipomas greater than 10 cm in size.1 They are commonly diagnosed clinically, but an indication for biopsy would include a firm, rapidly enlarging mass. Lipomas can be managed conservatively or excised.1 Other treatments include liposuction.2 Transformation of lipomas into liposarcoma is rare. Findings indicative of liposarcoma on MRI include male sex, advanced age, thick septa, nodularity, reduced fat composition and invasion of underlying tissue.3 Histologically, main features of liposarcomas include immature adipocytes and multivacuolation with indented and hyperchromatic neuclei.4
Learning points
Lipomas are usually small in size, with a soft consistency, but, in some cases, they can be relatively firm and impressive in size.
While lipomas can be clinically diagnosed, a differential diagnosis of liposarcoma must be considered in a firm, painless, enlarging subcutaneous lesion. This is an indication for biopsy.
MRI is a useful imaging modality in distinguishing lipomas versus liposarcomas.
Acknowledgments
The authors wish to thank the Mater Hospital Clinical Photography, Pathology and Radiology Departments.
Footnotes
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.