Article Text

Summary
Use of a postpartum intrauterine contraceptive device (PPIUCD) is a highly effective, reversible and long-acting family planning method that can be initiated in the immediate postpartum period, especially in lactating women. PPIUCDs have been inserted in more than 65 000 women worldwide and the numbers are increasing with many countries introducing PPIUCDs as part of their family planning programme. As the numbers of PPIUCD insertions are increasing, we are getting wiser regarding complications of this procedure. One of the less-understood entities is a malpositioned PPIUCD, a situation where the IUCD is present inside the uterus but its placement is eccentric and a part or the whole of it may be embedded in the myometrium. It can present as lost strings or as a failure to remove the intrauterine device. We present a series of cases with malpositioned PPIUCDs and their management.
Statistics from Altmetric.com
Case presentation
Case 1
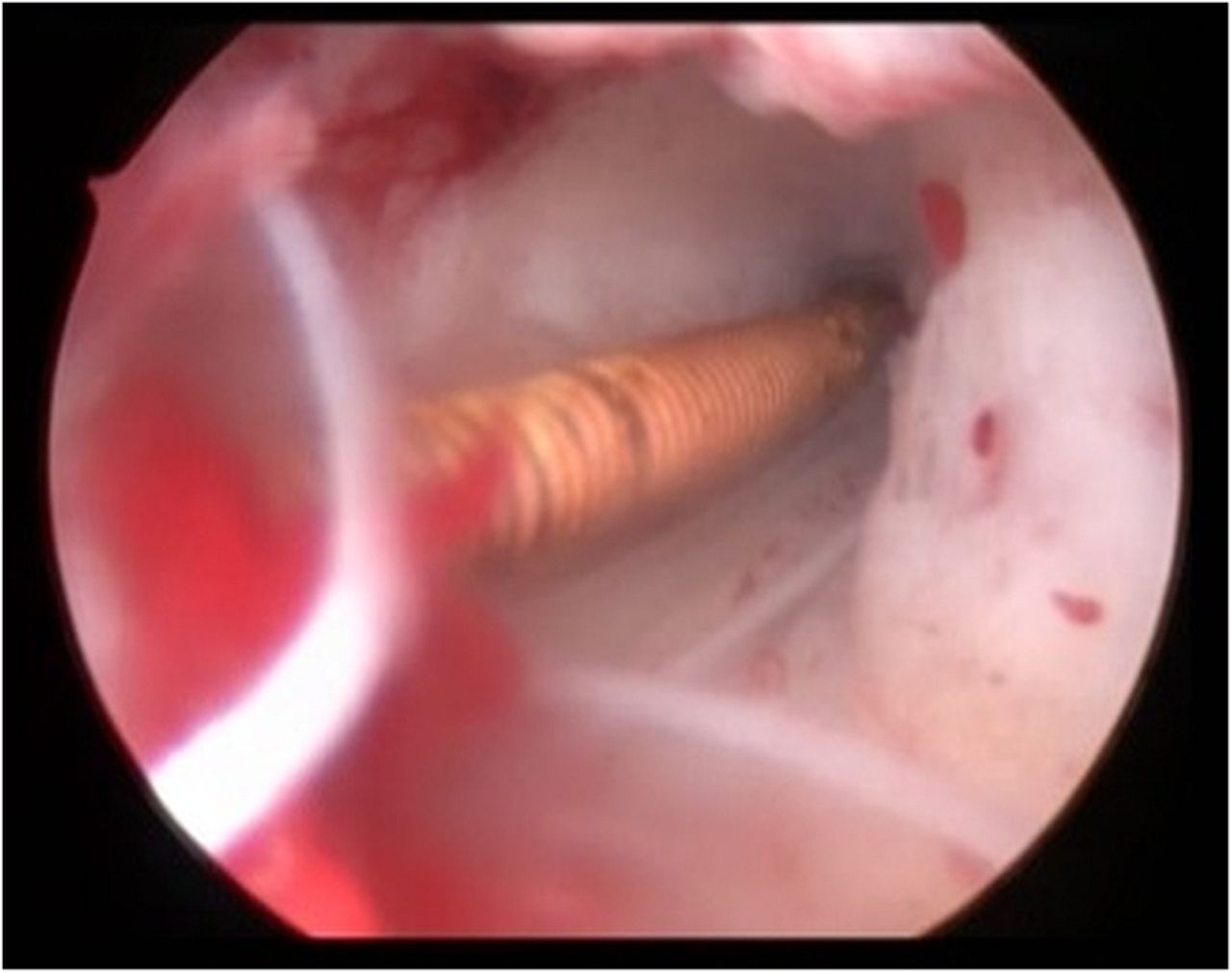
A 22-year-old woman with parity 1 presented with frequent periods. She had a postpartum intrauterine contraceptive device (PPIUCD) inserted after vaginal delivery 9 months earlier. General and systemic examination was normal. On speculum examination, the IUCD threads were not seen. Bimanual vaginal examination was normal. Ultrasonography (USG) of the pelvis showed the IUCD in uterus at an oblique orientation. The patient underwent hysteroscopy, confirming a malrotated IUCD, that is, a horizontal arm in vertical position with thread curling around, which was subsequently removed in the same sitting (figure 1).

Hysteroscopic image showing a malrotated intrauterine contraceptive device (IUCD) with thread curled in the uterine cavity.
Case 2
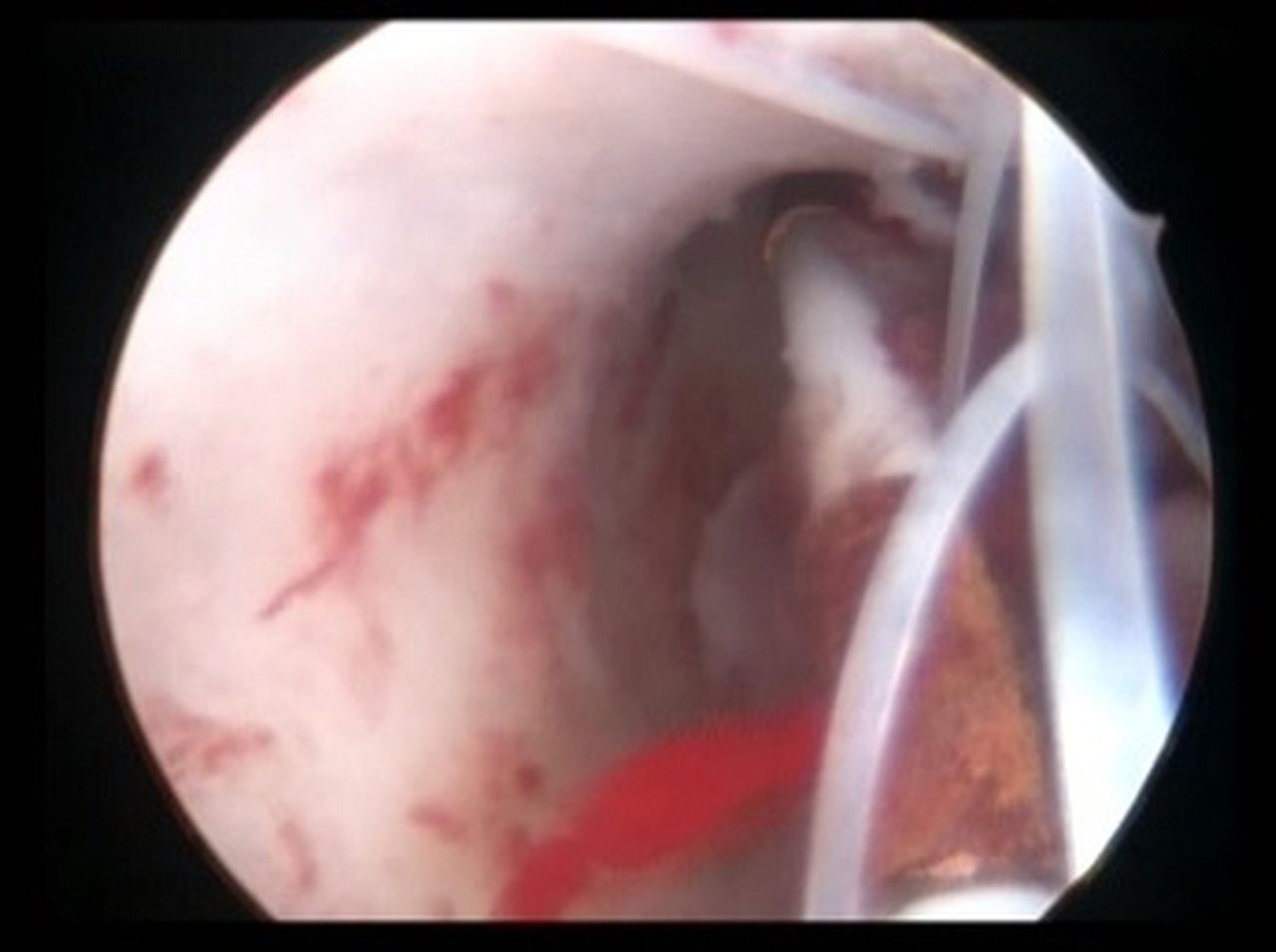
A 37-year-old woman, para 3, presented with absent IUCD threads. She had a PPIUCD inserted 15 months earlier, following vaginal delivery. Her periods were regular and she had no other problems. Speculum examination did not show IUCD threads. Bimanual vaginal examination was normal. The pelvic X-ray showed a horizontally lying IUCD (figure 2). USG findings revealed the IUCD inside the uterine cavity embedded in myometrium. On hysteroscopy, the vertical limb of the IUCD was oriented towards the right cornua. The horizontal arms of the IUCD were hanging in the uterine cavity towards the left (figure 3). The IUCD was removed hysteroscopically.

Pelvic X-ray showing a horizontally lying Cu T in the uterine cavity.
Hysteroscopic view showing a vertical arm of a Cu T 380 A entering a uterine cornua.
Case 3
A 29 year-old women, para 3, with two previous lower segment caesarean sections (LSCS) presented with non-visualisation of IUCD threads and irregular bleeding per vaginum. She had had the PPIUCD inserted during caesarean section. On speculum examination, the threads were not seen. Vaginal examination revealed a normal uterus and adnexa. USG showed the IUCD embedded in the myometrium (figure 4). Hysteroscopy revealed the IUCD embedded in the left lateral wall of the uterus; the IUCD was removed.

Ultrasonography showing an embedded Cu T in uterine myometrium.
Case 4
A 25-year-old woman, P1L1, who had undergone a LSCS 1 year prior, presented for removal of an IUCD that she had had inserted during the caesarean section. Speculum examination revealed a thread in the cervical tissue in place of cervical os (figure 5). Ultrasound revealed the IUCD embedded in the cervical tissue and lower part of the uterine wall. The IUCD was removed by pulling the thread carefully.

Speculum examination showing an intrauterine contraceptive device (IUCD) thread (arrow) passing through cervical substances.
Global health problem list
A malpositioned IUCD is one of the less reported complications of postpartum insertions, where the patient can present with
Missing IUCD threads on follow-up examination;
Abnormal position of IUCD on USG;
IUCD embedded in the myometrium or cervical tissue;
Menstrual abnormalities.
Global health problem analysis
Contraceptive options are limited in the postpartum period, especially for lactating women. An international survey conducted in 52 countries found that children conceived <24 months apart had a higher risk of mortality.1 It also revealed that with decreasing birth intervals, there is a higher incidence of malnutrition and stunting of growth. In order to address this high unmet need for postpartum contraception, many countries, including India, have initiated PPIUCD insertion in recent years. This initiative aims to improve pregnancy spacing, thus contributing to improved maternal and child healthcare, especially in the context of developing countries.
PPIUCD insertion involves the insertion of a Cu T 380 A (provided free of cost by the Government of India) in the first 48 h of delivery of fetus. This device has high acceptability rates and low incidence of complications.2 There are three kinds of postpartum insertions of IUCDs: postplacental (inserted within 10 min of delivery of placenta), intracaesarean and within 48 h postpartum.3 Postplacental and intracaesarean constitute 79% of postpartum IUCD insertions in India.
PPIUCD insertion has been observed to have an impact on the acceptance of long-acting reversible contraception, especially interval IUCD. Unless the complications are well understood and women counselled accordingly, side effects can, similarly, have a negative impact on attitude towards IUCDs. It is therefore imperative that the different types of complications be reported and analysed. The commonly reported side effects of PPIUCDs are an increase in menstrual bleeding, spotting and abdominal cramps. Rarely, PPIUCDs can result in expulsion of the device. These side effects usually subside over a variable period of time.3 Sometimes, a normally seen thread may be associated with an embedded IUCD, where it would be difficult to remove the IUCD.4
A malpositioned IUCD is a condition where, although the IUCD is present inside the uterus, its placement is eccentric and part or the whole of it may be embedded in the myometrium. It can present as lost strings or as a failure to remove the IUCD. The management and counselling of women in this condition is a challenge for the general physician as well as the trained gynaecologist. Studies have noted the incidence of lost strings from PPIUCDs to vary from 5.3% to as high as 24%.2 ,5 ,6 The majority (91.8%) of lost strings curl inside the cervical canal and can easily be found.7
Marchi et al8 reported that, in cases of missing threads with interval IUCD, 98% of IUCD were normally positioned, in 1.2% the IUCD was expelled and in 0.7%, the IUCD had caused uterine perforation. The postplacental PPIUCD is a relatively new concept, therefore, a close watch should be kept on potential complications arising from it. As the acceptance of PPIUCD is expected to increase, there will be an increased incidence of rarer complications, especially lost strings and the need for USG of the pelvis to determine the position of the IUCD.
The reason for the malpositioning in cases of PPIUCDs use could be a large uterine cavity and contraction of the uterus during the process of involution. Because of these two reasons, the IUCD direction may easily change, as in case 2, where the vertical arm went into one of the cornual ends. The ultrasound appearance in this case, however, was of an embedded IUCD, but in actuality, it was the opposing walls of the cornual end that gave the appearance of a device embedded in the myometrium. The reason for embedded IUCDs in cases 3 and 4 could be the malpositioned vertical arm, which continuously probes the myometrium during the lactation period, when the uterus is soft, and embedding in a part of it.
To avoid this complication, one must follow a few points while inserting an IUCD.
During caesarean section, the strings of the IUCD should be directed towards the cervical canal.
During vaginal delivery, the device should be placed high at the fundus, and, while withdrawing the Kelly's forceps, the thread should not be pulled.
The IUCD should be held at the intersection of the T while insertion so as not to deviate its axis.
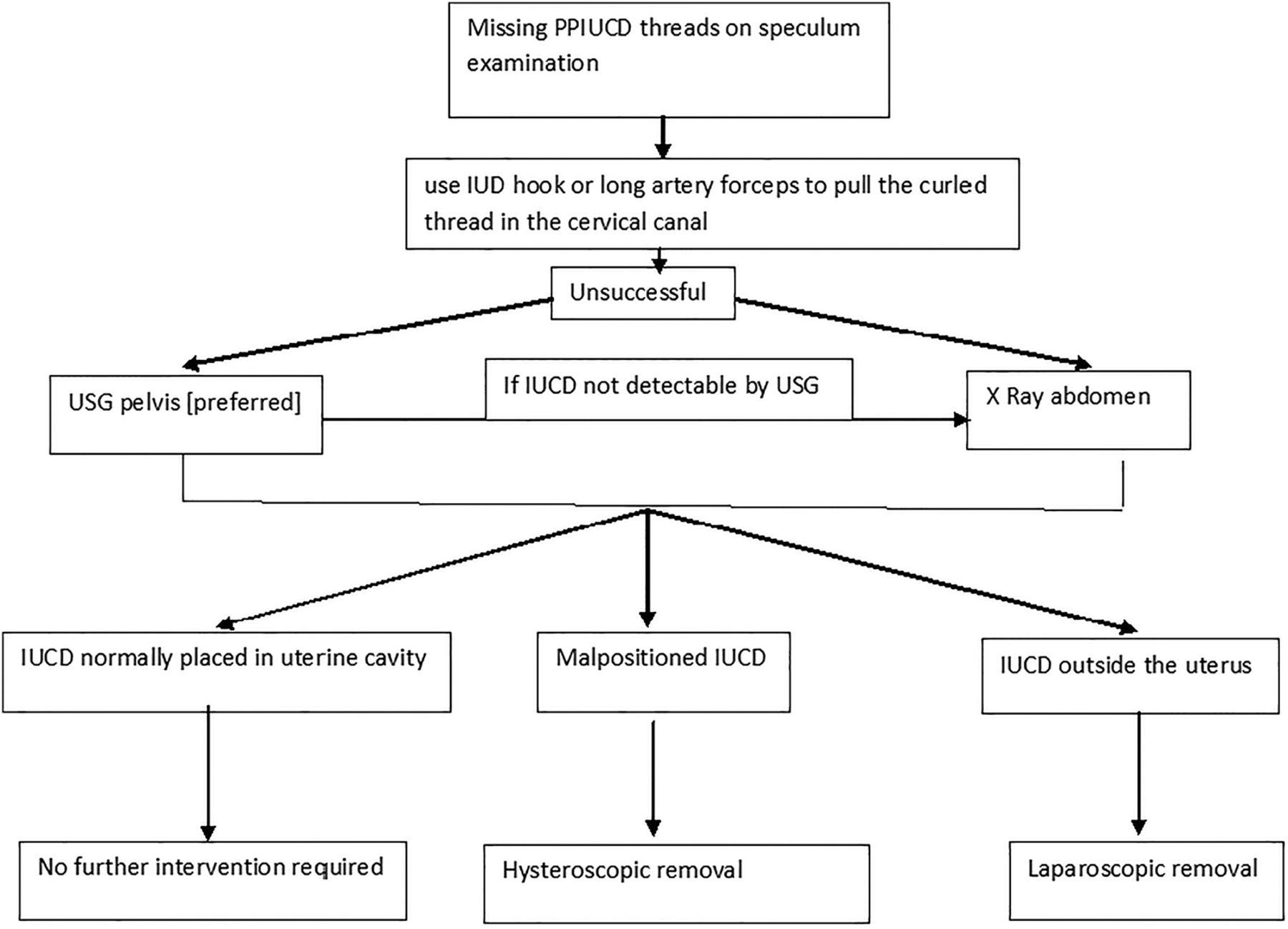
As shown in figure 6, it has been suggested that, in case of missing or shortened threads, the cervical canal should be probed first, using a cytobrush or an IUD hook, to locate the retracted threads.9 If this fails, one can proceed with pelvic USG or abdominal X-ray. In the event of a malpositioned or embedded device, one must carry out hysteroscopic removal of the IUCD, as there are increased chances of pregnancy in the case of a malpositioned IUCD.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic presentation of management of a misplaced PPIUCD (USG, ultrasonography; PPIUCD, postpartum intrauterine contraceptive device).
We found that, as part of initial evaluation, USG of the pelvis can be performed. However, at times, the USG may incorrectly show the PPIUCD in supposedly proper position. Davey et al10 found that adhesion formation starts within a few days of tissue injury and develops within a week. Hysteroscopy yields the correct picture and should be the preferred modality to remove an IUCD, compared with blind removal as, at times, removal may be complicated by adhesions and fibrosis.
Learning points
A malpositioned IUCD is a relatively less reported complication of postplacental postpartum IUCD.
Ultrasound should be performed as an initial diagnostic evaluation in the event of missing threads.
In women with PPIUCDs and missing threads, one should always consider the possibility of a malpositioned IUCD, because the radiological findings may not always give an accurate picture.
Hysteroscopy is a good modality for the removal of malpositioned IUCDs.
Footnotes
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.