Article Text

Summary
The safety of laser pointers is a major public health issue since class I and II laser pointers are available worldwide and used as toys by children despite several reports cautioning such use. Here we present the first case of retinal injury caused by the laser beam of a toy laser pointer operated by a school boy and directed via the rear-view mirror of a bus into the eye of the driver. This case emphasises the great importance of cautious and appropriate use of low-energy laser pointers. Laser pointers of any class should not be made available to children because they are unlikely to understand the risks of such lasers when using them in play.
Statistics from Altmetric.com
Case presentation
A 44-year-old public bus driver who was previously healthy with a full bilateral best-corrected visual acuity (BCVA) of 1.0 (20/20) was exposed to the laser beam of a toy laser pointer handled by a school boy (figure 1B) from a distance of about 16.5 m (figure 1A). The beam was reflected in the inside rear-view mirror of the bus, and the driver stared into the laser light several times in order to locate the person holding the laser. Immediately after this exposure the driver complained of blurred vision in his right eye that had persisted for 6 months when the first complete ophthalmological examination was carried out.

(A–D) Reconstruction of the laser beam reflection in the public bus (A). The laser beam travelled 16.5 m from its source into the driver's eye when he viewed it several times via the inside rear-view mirror. (B) Typical handheld toy laser pointer with an output power of 5 mW. (C) Maximum permissible exposure (MPE) as power density versus exposure time for various wavelengths. (D) Maximum allowed exposure time to a laser with an optical power of 1 and 5 mW.11
The maximum permissible power density of laser beams versus exposure time for various wavelengths is shown in figure 1C, while the maximum allowed exposure time of a laser pointer with output powers of 1 and 5 mW is shown in figure 1D.
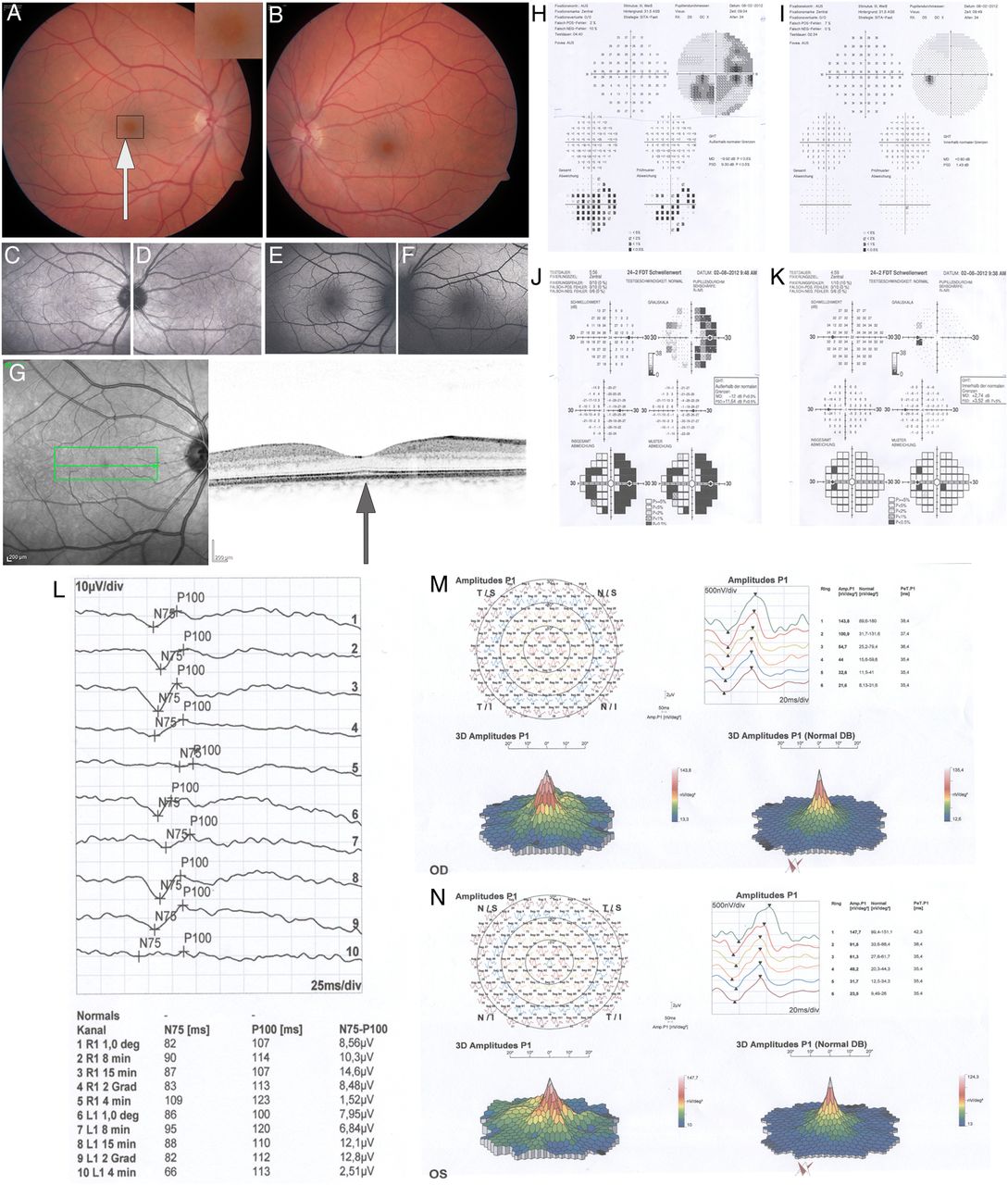
Upon presentation, the driver's BCVA was 0.8 OD and 1.0 OS. Slit-lamp biomicroscopy revealed no abnormalities in the anterior segment of either eye. Intraocular pressure was normal. Dilated ophthalmoscopy revealed barely visible retinal pigment epithelium disturbances within the temporal macula of his right eye (figure 2A) and no pathological changes in his left eye (figure 2B). A paracentral scotoma extended at up to 25° of eccentricity in his right eye (figure 2H,J), with a normal visual field in his left eye (figure 2I,K). Optical coherence tomography revealed spot-like retinal pigment epithelium disturbances temporal to the fovea of the right eye (figure 2G), with no abnormalities in his left eye (not shown). Infrared and autofluorescence images of both eyes showed normal macula patterns (figure 2C–F). Visual evoked potentials were normal and identical in both eyes (figure 2L). However, multifocal electroretinography (mfERG) showed paracentral focal disturbances with altered sum peak in the right eye (figure 2M). The mfERG of his left eye was normal (figure 2N).

{kind=link}
{kind=link}
Fundus photography of the right eye (A) and left eye (B) with subtle pigment epithelium disturbances temporal to the fovea of the right eye. (C–F) Infrared image and autofluorescence photographs of both eyes without detectable changes in the central retinas. (H–K) Visual fields of the right eye (H and J) and left eye (I and K). A clear nasal paracentral scotoma in the left eye was detected with a Humphrey 30–2 device (H) and microperimetry (J). The visual field of the left eye was normal. (I and K) (G) Optical coherence tomography of the right eye with subtle pigment epithelium defects and interruption of the photoreceptor layer (arrow) correlating with the location of the paracentral scotoma in the right eye. The configuration of the left eye was normal (not shown). (L) Visual evoked potentials were normal in both eyes. (M and N) Multifocal electroretinography (mfERG) of the right eye (M) with focal paracentral disturbances and sum-peak reduction (left) compared to the reference (right) and the normal mfERG of the left eye (N) compared to the reference (right).
Global health problem list
The subjective complaints and objective ophthalmological findings of this patient were consistent and strongly suggested that the repetitive exposure of the eye to the reflected laser spot 6 months previously had caused subtle but detectable injury to the macula. Although the exact energy of the handheld laser pointer was not determined, the descriptions and reports of those involved suggested that it was a class II or class 3R laser device (1 or 5 mW). In addition, the bus driver had looked at least three or four times into the mirror in order to locate the laser source, implying that he had received a minimum of least 10 s of cumulative exposure to the laser beam.
Most cases of laser-induced maculopathies are based on accidental exposure to high-energy class IV lasers with laboratory, medical, recreational,1–3 or civil and military applications.4 Lower-energy class IIIa lasers pose little risk of retinal damage5 when used properly, but there are case reports of retinal damage caused by direct exposure to class IIIa commercial laser pointers,6–9 and to higher-energy class IIIb laser pointers.8–10 The risk of damage to the retina varies with the energy of the laser device and the duration and number of exposures. Repeated exposure to a low-energy green laser pointer can result in maculopathy and delayed choroidal neovascularisation.4 Handheld laser pointers typically have output energies in the range of 1–5 mW; the output power of toy laser pointers is limited to 1 mW.
Global health problem analysis
This report is the first to show that repeated viewing of even the reflected beam of a low-energy laser may cause damage to the macula in an unprotected eye. The subject reported that the laser beam was red, and so it was most likely a handheld laser pointer emitting at a wavelength of around 650 nm. The divergence of the laser beam from such a device is about 1 mrad, so the beam diameter increases by around 1 mm/m distance from the laser. Thus, for a distance of 16.5 m between the laser source and the driver's eye, the beam would have had a diameter of about 16 mm. About 63% of the laser energy is located within an ‘effective radius’, meaning that the effective diameter of the beam that reached the driver's eye was 11–12 mm.
Learning points
We suggest that no laser pointers of any class are made available to children, since they are unlikely to understand the risks of permanent retinal damage.
For the safety of users and the general public, even low-energy handheld laser pointers should not be sold to children.
Footnotes
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.