Article Text

Statistics from Altmetric.com
Description
Thrombosis of multiple coronary arteries at the same time is an uncommon angiographic finding during the course of ST-segment elevation myocardial infarction (STEMI). This clinical condition usually leads to cardiogenic shock or even sudden cardiac death. We present a case of a man who presented with STEMI due to simultaneous occlusions of the left anterior descending artery (LAD) and right coronary artery (RCA).
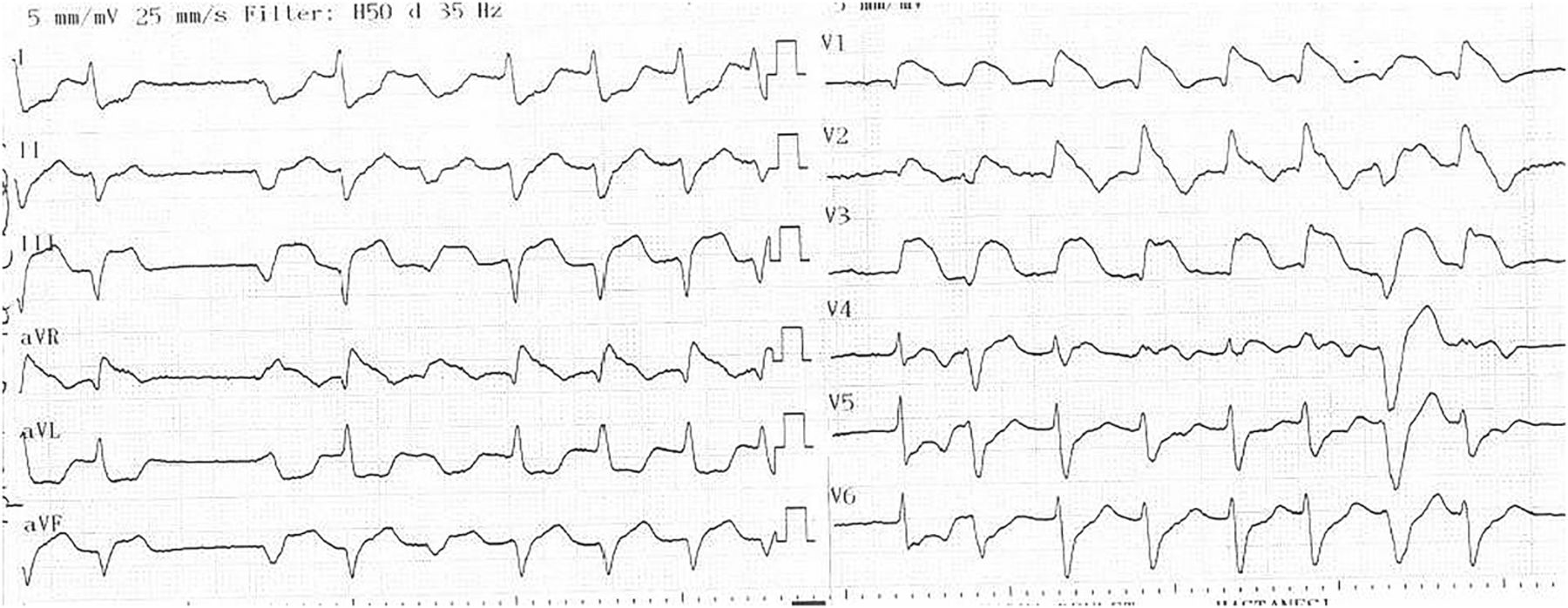
A 57-year-old man was referred to our emergency department due to central chest pain and ST-segment elevations in anterior and inferior leads (figure 1). He did not have any particular diseases or well-described risk factors in his medical history. Based on ECG findings, his LAD was thought to be the cause; however, his emergent coronary angiography revealed thrombi in the LAD as well as RCA. The LAD (videos 1⇓–3) and RCA (videos 4⇓–6) were successfully treated with stent implantations. The patient's laboratory tests, which included antithrombin III, protein C and protein S deficiencies, and activated protein C resistance, did not indicate any coagulation disorders. Lupus anticoagulant, anticardiolipin IgM and IgG were all negative. The patient's platelet count was 213 000/mm3. Echocardiography performed before the procedure did not reveal any thrombus in the left ventricle and the patient did not have a history of atrial fibrillation before the acute coronary event.
{kind=link}
ST-segment elevations in inferior and anterior leads.
Proximal total occlusion of left anterior descending artery.
Endeavour resolute 3.0/15 mm drug-eluting stent (Medtronic Inc, Minneapolis, Minnesota, USA) implantation at 16 ATMs.
Final angiographic injection of left anterior descending artery.
Proximal total occlusion of right coronary artery.
Ephesos 4.0/18 mm bare metal stent (Alvimedica, İstanbul, Turkey) implantation at 17 ATMs.
Final angiographic injection of right coronary artery.
Different possible underlying conditions causing double coronary artery occlusions during the course of STEMI have been suggested, such as cocaine use, a hypercoagulable state and essential thrombocytosis.1 However, the underlying mechanism still remains unclear in most of these patients, as in our case. Previous studies conducted via angioscopy and intravascular ultrasound demonstrated that multiple atherosclerotic plaque ruptures are frequent during the setting of acute coronary events and can be observed in different coronary vessels. Recently, Karabay et al2 also reported anterior and inferior myocardial infarctions in a patient due to simultaneous total occlusions of both the LAD and RCA. In 2015, Mahmoud et al conducted a systematic review on simultaneous multivessel thrombosis during STEMI, including 29 articles, which totally yielded 56 patients. They revealed that simultaneous thrombosis of the LAD and RCA was the most common angiographic finding in this clinical setting.3 It should always be kept in mind that coronary arteries must be examined properly during emergent percutaneous coronary interventions, especially if the patient presented with cardiogenic shock or sudden cardiac death, or if multiple arteries are suspected to be the cause. Further studies are required in order to evaluate contributing factors causing extensive thrombosis in multiple coronary vessels in acute coronary syndromes.
Learning points
Despite the tendency to blame a single lesion as being the cause, ST-segment elevation myocardial infarction involving double coronary artery occlusions may occur. Therefore it is crucial to accurately diagnose the clinical condition and determine the appropriate treatment since most of these patients are hemodynamically and clinically unstable.
Footnotes
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.