Article Text

Statistics from Altmetric.com
Description
A 46-year-old woman presented with severe upper abdominal pain and vomiting 12 h post-endoscopic retrograde cholangiopancreatography (ERCP) and sphincterotomy for choledocholithiasis. The patient also described a sensation of ‘crackling in the neck’ on head rotation. On examination, the patient was stable and afebrile, and had pain in the right hypochondriac region. She had subcutaneous crepitations in the right side of the neck and chest. Blood results showed white cell count 15.5×109/L, C reactive protein 13.7 mg/L, amylase 55 IU/L, alanine transaminase 46 IU/L and alkaline phosphatase 300 IU/L; all other blood tests were normal.
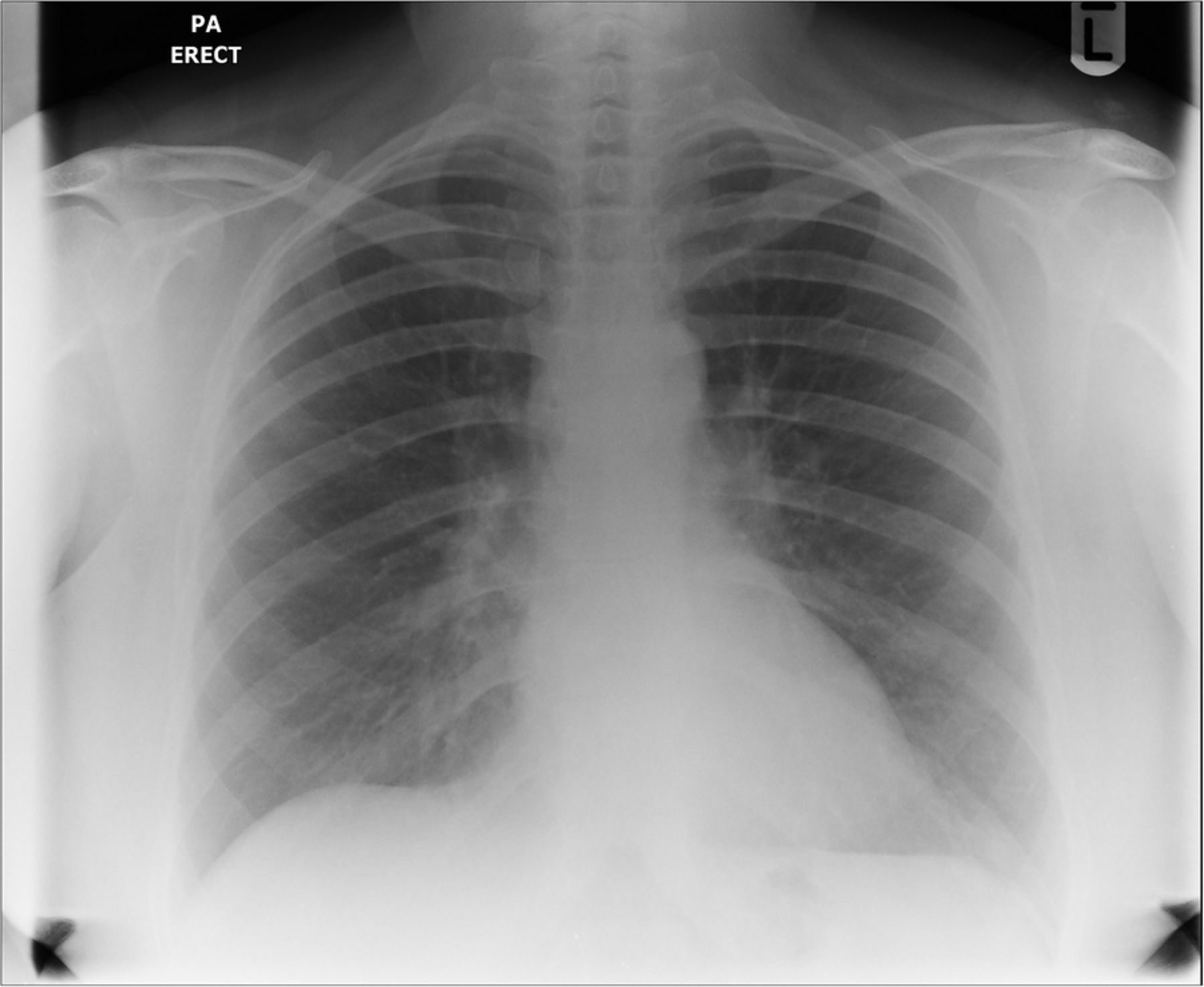
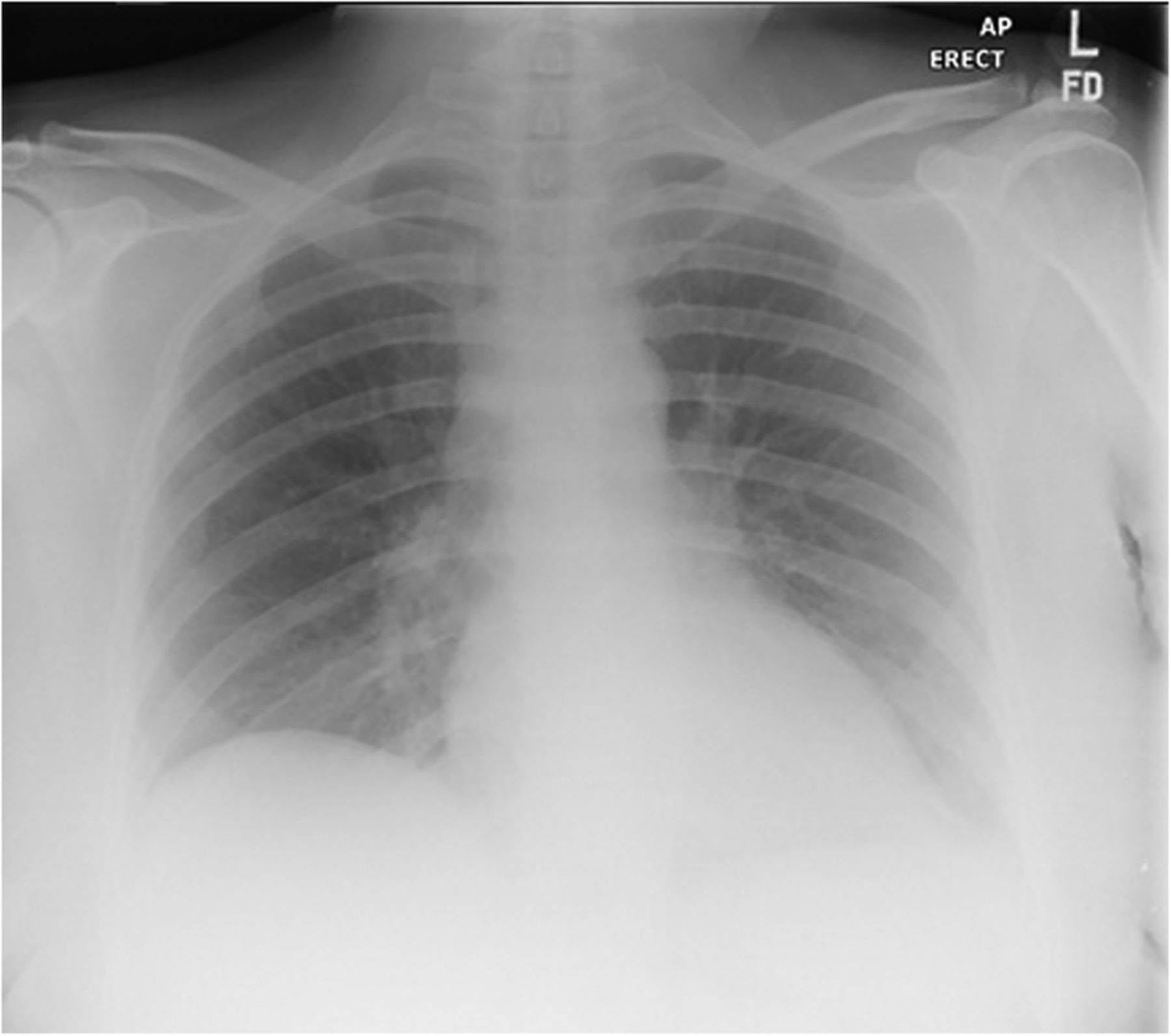
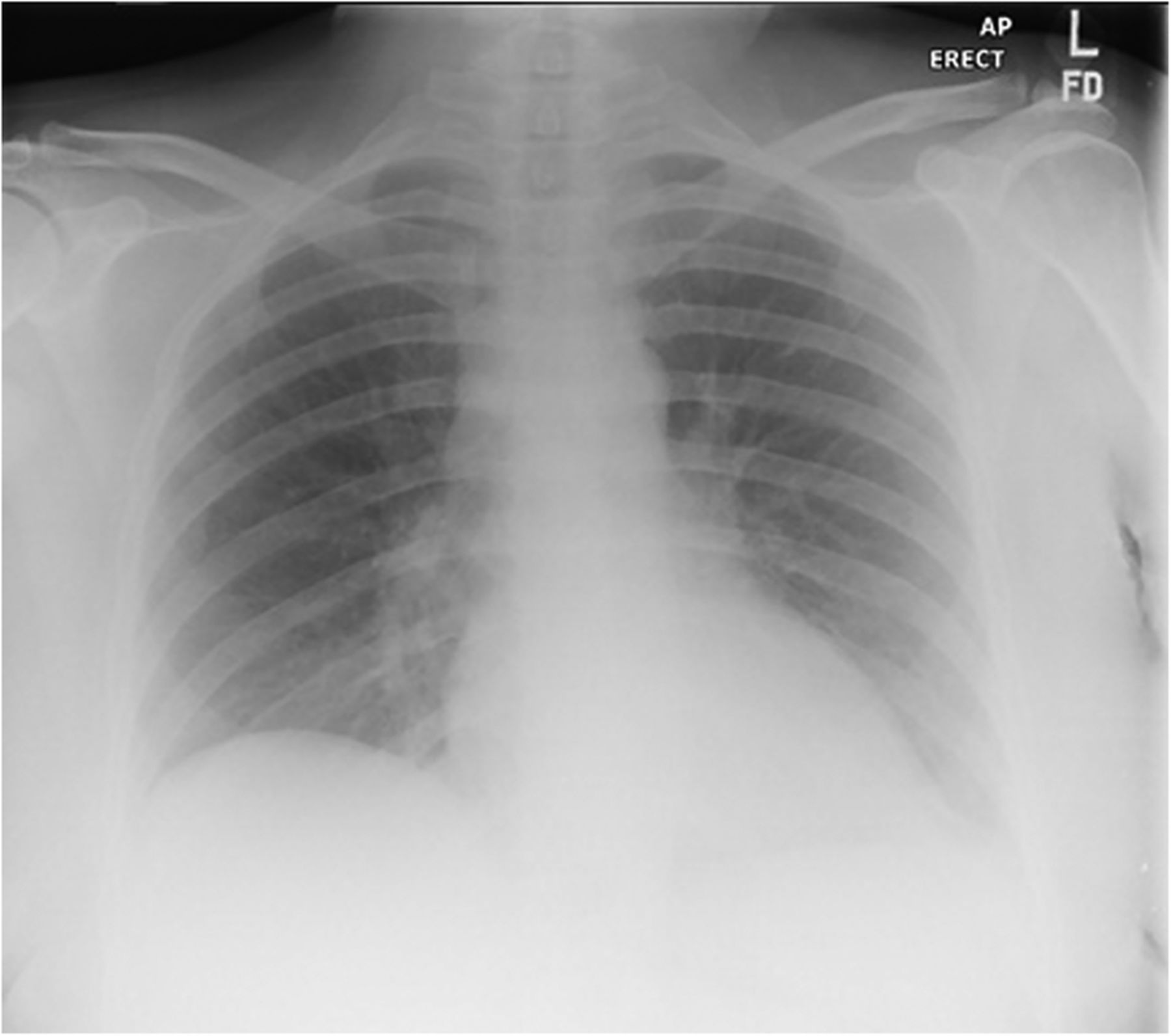
An erect chest radiograph demonstrated a pneumopericardium, pneumomediastinum and surgical emphysema in the root of the neck (figure 1). An abdominal radiograph showed a large amount of retroperitoneal free air in the upper abdomen and surrounding the kidney—suggesting a duodenal perforation (figure 2). These findings were not present on the preprocedure film (figure 3).

Abdominal radiograph demonstrating a large amount of retroperitoneal air, in particular, surrounding the kidneys.

Chest radiograph demonstrating extension of the retroperitoneal air, which appears similar to a pneumopericardium. There is evidence of surgical emphysema in the root of the neck, which explains the ‘crackling in the neck’.
Repeat chest radiograph demonstrating reabsorption of the free air.
The ERCP, performed by an experienced endoscopist, had been without apparent difficulty. During the procedure, a stone was identified as obstructing the distal common bile duct (figure 4). A sphincterotomy was performed and a biliary stent placed (figure 5).

Fluoroscopy image demonstrating successful cannulation of the common bile duct stricture after sphincterotomy.

Fluoroscopy image demonstrating successful cannulation of the common bile duct stricture after sphincterotomy.
The patient was managed conservatively with a nasogastric tube, intravenous fluids and antibiotics. She made a full recovery and was discharged 4 days later. A repeat chest radiograph on discharge showed reabsorption of the free air (figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Erect chest radiograph demonstrating resolution of intraperitoneal free air.
The incidence of perforation post-ERCP has been investigated by Howard et al, who performed a retrospective analysis of 6040 ERCPs. The group demonstrated that, of the 2874 patients (48%) who had a sphincterotomy, 40 patients (0.6%) went on to develop perforation.1 The group also reported an overall ERCP complication and mortality rate of 8.2% and 1.3%, respectively.
Patients with a duodenal perforation often present with abdominal pain and vomiting, which mimics the more common complications of acute pancreatitis.2 Serum amylase and imaging, ideally CT, are important in investigating and differentiating these complications.2
The management of duodenal perforation post-ERCP is controversial. Howard et al1 demonstrated successful conservative management in 36 of 40 patients with a perforation. The group suggests a risk stratification based on mechanism of injury, site of perforation and timing of diagnosis, to determine the need for operative intervention. Stapfer et al3 reviewed 14 cases of ERCP-related perforations and, in stable patients, concluded that conservative management was superior to surgical intervention. Operative management is patient-specific but often involves drainage of leaked contents, repair of duodenal defects and a cholecystectomy.3
Learning points
Duodenal perforation is a rare (0.6%) but important complication of endoscopic retrograde cholangiopancreatography (ERCP).
Chest and abdominal radiographs are useful in assessing post-ERCP complications.
In stable patients, conservative management of duodenal perforation post-ERCP is preferred.
Footnotes
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.