Article Text

Statistics from Altmetric.com
Description
A 33-year-old Caucasian woman with Class 1 idiopathic pulmonary arterial hypertension (PAH) managed on tadalafil, ambrisentan, treprostinil, digoxin and diuretics presented with progressive dyspnoea and orthopnoea since 2 weeks. Cardiac examination revealed hypotension, tachycardia, pulsus paradoxus, jugular venous distension, muffled heart sounds, loud P2 and holosystolic murmur at left-lower sternal border. Transthoracic echocardiogram demonstrated a large circumferential pericardial effusion (PCE) with diastolic left atrial (LA) collapse and uncollapsed right atrium (RA; figures 1 and 2). Severe RA enlargement, severe tricuspid regurgitation, elevated right ventricular (RV) systolic pressure (170 mm Hg) and dilated non-collapsible inferior vena cava were noted. RV demonstrated severe dilation and systolic dysfunction with paradoxical septal motion. Mitral valve demonstrated increased respiratory flow variation (figure 3). Urgent pigtail catheter placement and drainage of 200 mL provided haemodynamic improvement. Gradual drainage of 2.3 L over 15 days was performed, with steady improvement in LA filling (figure 4). Serological and microbiological studies were unrevealing and the patient was referred for pulmonary rehabilitation, pending heart–lung transplantation.

Transthoracic echocardiogram (parasternal long-axis view) showing left atrial and ventricular collapse as an atypical sign of cardiac tamponade.

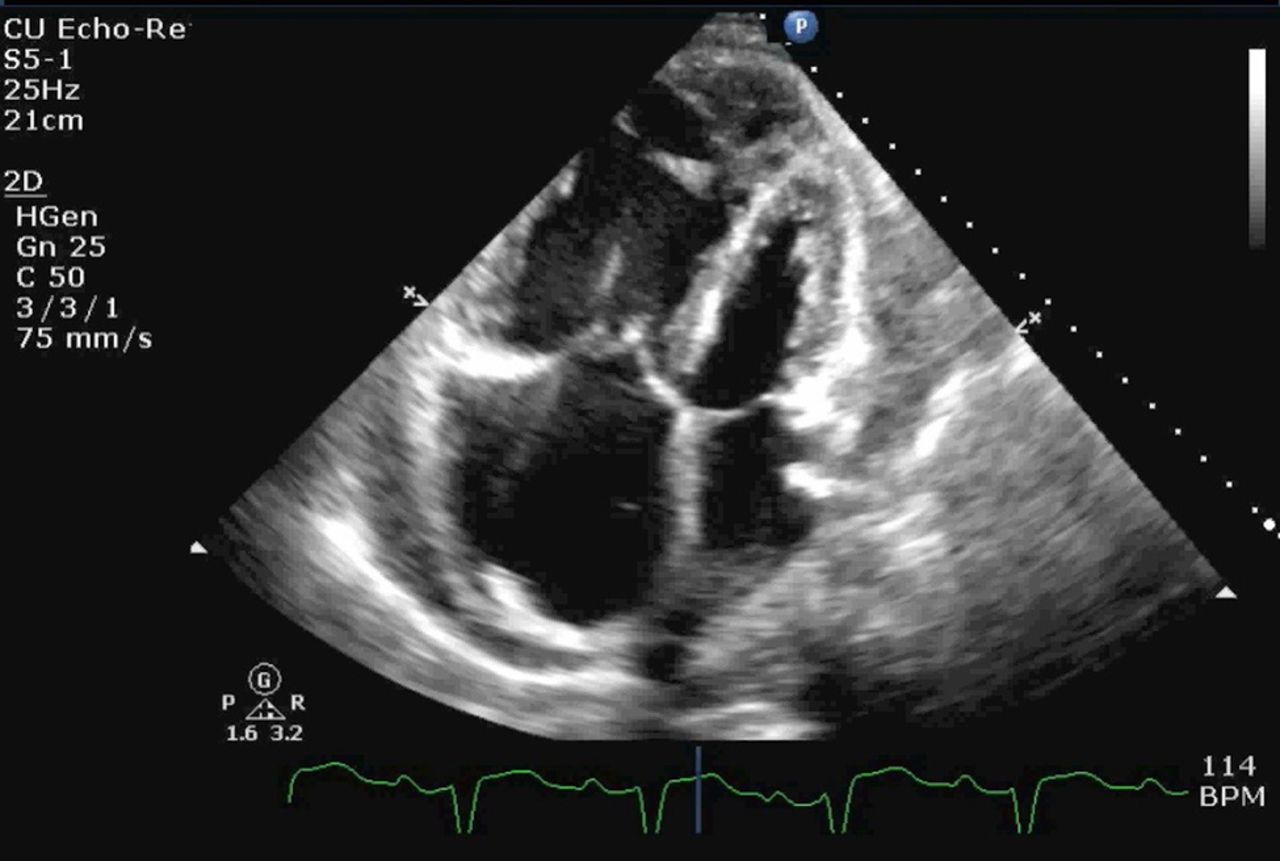
Transthoracic echocardiogram (apical four-chamber view) demonstrating systolic left atrial and ventricular collapse.

Transthoracic echocardiogram (apical four-chamber view) demonstrating respiratory variation in mitral inflow.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Transthoracic echocardiogram (apical four-chamber view) at discharge demonstrating improvement in left atrial volume.
In the setting of PAH, PCE is noted in 15–65% and is an independent mortality predictor.1–3 PCE resulting in cardiac tamponade is noted only in 0.02% of PAH cases and causes significant haemodynamic and echocardiographic alterations due to high RA pressures.1 ,3 ,4 Postulated mechanism is venous/lymphatic obstruction with consequent cytokine release.2 ,3 Atypical signs of tamponade include isolated LA/left ventricular collapse and increased respiratory variation of transmitral inflow.4 Rapid drainage has high peri-procedural mortality due to RV decompensation.2 ,3 ,5 Gradual drainage, as in our patient, may be safer resulting in haemodynamic improvement.1
Learning points
Pericardial effusion (PCE) in pulmonary artery hypertension (PAH) is rare and is an independent mortality predictor.
Only 0.02% of patients with PAH have a significant PCE causing cardiac tamponade that frequently presents atypically due to elevated right-sided pressures.
Gradual drainage of PCE is advantageous in conferring haemodynamic stability.
Acknowledgments
The authors would like to thank Venkata M Alla, MD and Swapna Kanuri, MBBS from the Division of Cardiovascular Medicine, Creighton University School of Medicine for their critical evaluation and feedback on the manuscript.
Footnotes
Contributors SV contributed to evaluation of the patient, literature review, and drafting and finalising the manuscript. PRS contributed to evaluation of the patient and drafting of the manuscript.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.