Article Text

Statistics from Altmetric.com
Description
A 64-year-old woman with a history of diabetes mellitus, hypertension and previous unsuccessful coronary angiography via femoral approach presented to the emergency room with intermittent non-exertional chest discomfort.
Physical examination revealed symmetrical blood pressure of 150/90 mm Hg with equally weak pulses in all extremities and a soft systolic murmur over the sternum, appreciated on auscultation.
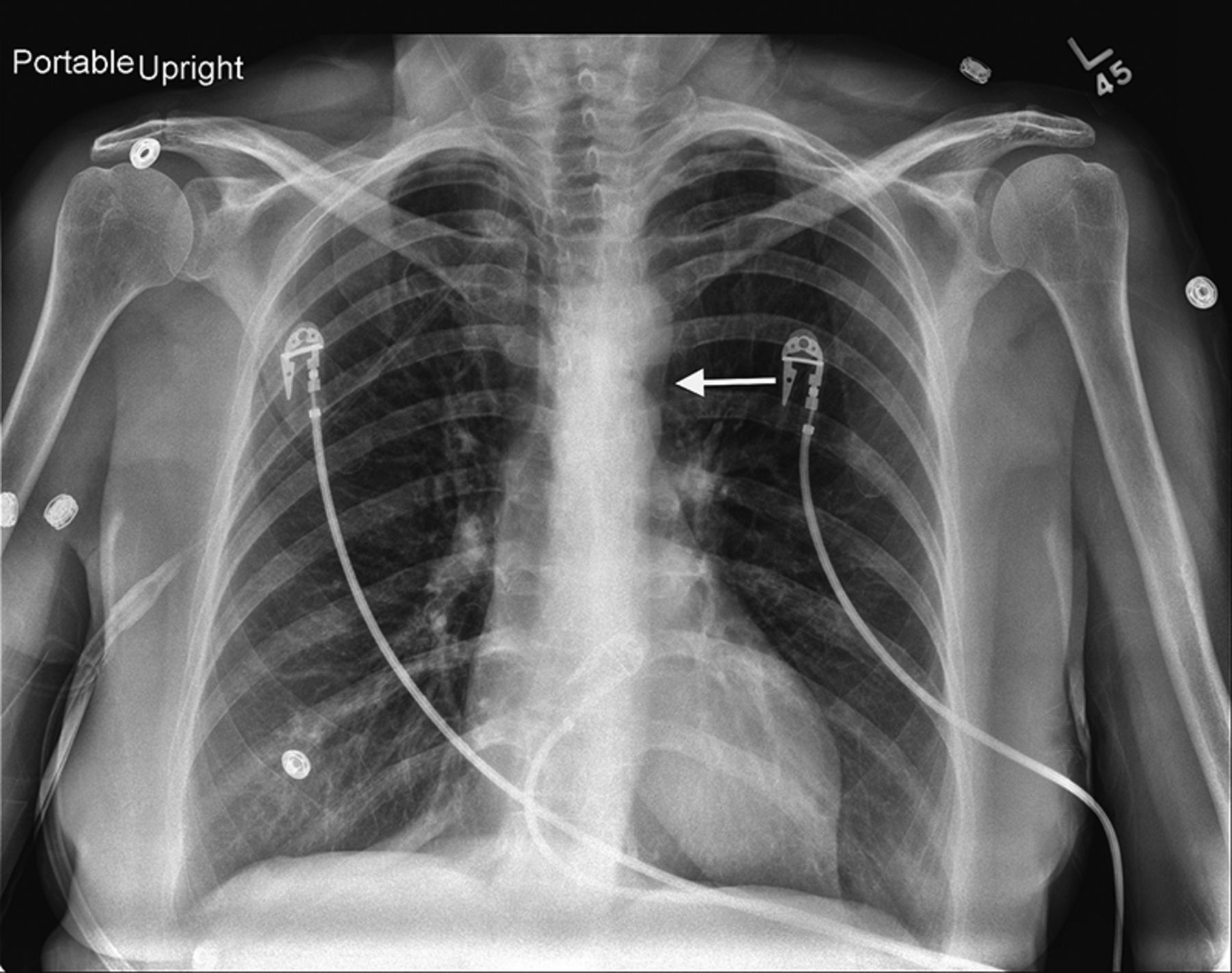
Chest radiograph (figure 1) revealed a double density in the aortic arch mimicking the number 3. Echocardiogram showed normal left ventricle ejection fraction and aortic valve structure without gradient. CT angiography (figure 2) of the chest further defined an elongated aortic arch, luminal narrowing distal to the left subclavian artery, post-stenotic dilation and pseudo-3 configuration. No collateral circulation or rib notching was noted, consistent with aortic pseudocoarctation.

Chest X-ray showing a double density in the aortic arch mimicking the number 3 (arrow).

{kind=link}
{kind=link}
CT angiography with three-dimensional reconstruction, showing an elongated and kinked aortic arch (dashed arrow), luminal narrowing distal to the left subclavian artery (arrow), post-stenotic dilation and pseudo-3 configuration.
Aortic pseudocoarctation is an uncommon congenital elongation and kinking of the aorta, without significant pressure gradient between extremities or increased collateral circulation, differentiating it from true coarctation. The diagnosis criteria were established by Gay and Young1 and include an abnormal posteroanterior chest roentgenogram (a left superior mediastinal density, in our case corresponding to the pseudo-3 sign), absence of pressure differential between the upper and lower extremities (or at most <25 mm Hg), no evidence of increased collateral circulation (eg, rib notching) and a definitive aortogram.
Pseudocoarctation is usually asymptomatic and, as in our case, can be recognised on routine chest X-ray films.2 Identifying this variant is essential as treatment is conservative.3 In our patient, a stress echocardiograph revealed no ischaemia, and was discharged on appropriate medical treatment.
Learning points
-
Aortic pseudocoarctation is a congenital elongation and kinking of the aorta that differs from true coarctation in that there is no significant pressure gradient between extremities or increased collateral circulation.
-
Pseudocoarctation is usually asymptomatic and can be recognised on routine chest X-ray films. Identifying this variant is essential as treatment is conservative.
Footnotes
-
Twitter Follow Jean Donet at @JeanDonet
-
Contributors ACF served as senior author and also as an attending physician taking care of the patient. GAH was also involved in the patient's care and, along with JAD and MS, was responsible for data collection, review of the literature and synthesis of the manuscript; the ACF supervised it.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.