Article Text

Statistics from Altmetric.com
Description
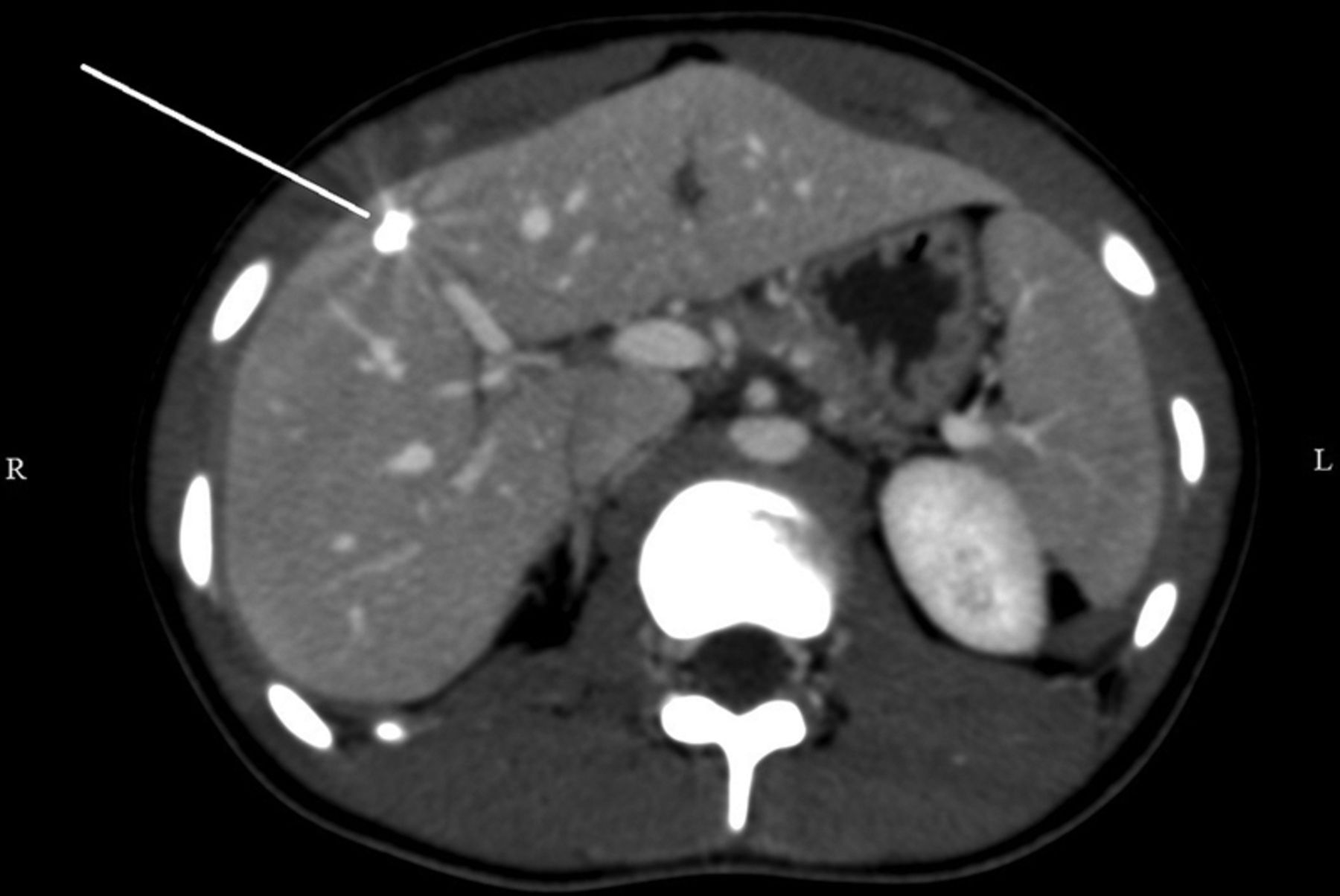
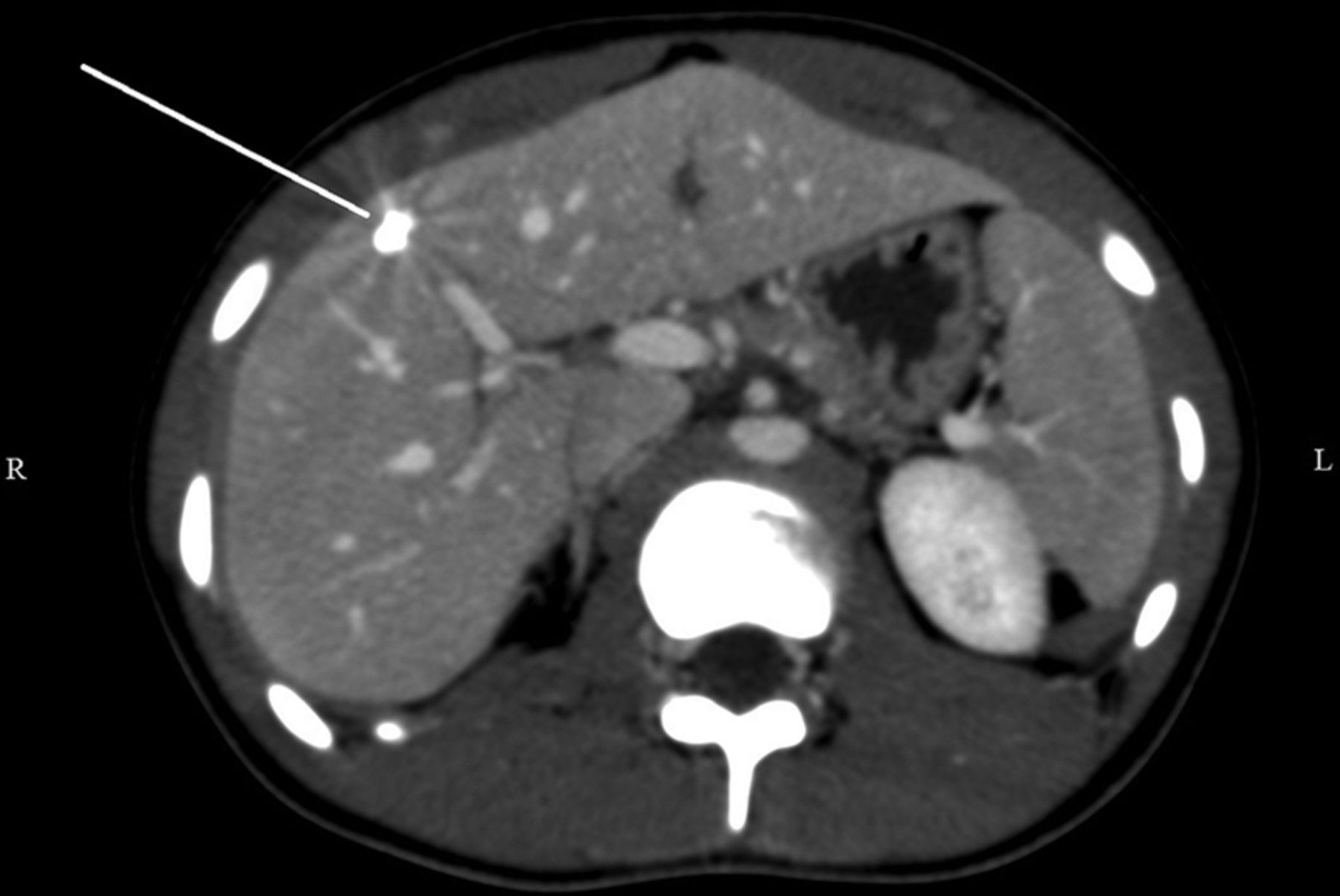
An adolescent girl with no remarkable medical history except several episodes of abdominal pain onsets, presented to the emergency department with pain in the right upper quadrant (RUQ) of the abdomen and nausea for 4 days. The pain was localised and aggravated by deep breathing, with no projections. Physical examination was unremarkable, except for tenderness during RUQ palpation. The patient had been accidently shot as a child. Detailed cutaneous examination revealed a scar on the posterior right side of the neck. CT of the abdomen (figures 1 and 2) revealed a subcapsular metal object between the fourth and eighth liver segments. A 17.8×5.6 mm rifle bullet was surgically removed. At the last follow-up visit, the patient had no residual pain.

CT scanogram of the abdomen showing a metallic object shaped like a bullet (white arrow).
{kind=link}
{kind=link}
CT of the abdomen with intravenous injection showing a metallic object at the junction between the fourth and eighth liver segments.
Bullet embolism is a rare complication after gunshot injury.1 It occurs when a projectile penetrates the initial tissue and a single vessel wall, and then rests within the lumen. Paradoxical embolism occurs when the bullet goes against the blood flow.1 Intravascular migration of foreign bodies is affected by blood flow, body position, gravity and vascular anatomy.2 For our case, a review of the events led us to assume that the bullet penetrated the posterior wall of the external right jugular vein and travelled with the blood flow in the superior vena cava, then against it in the inferior vena cava and in the intrahepatic venous system. Treatment of venous bullet emboli is frequently intravascular or by surgical removal, but remains controversial because the condition can be managed conservatively.3
Learning points
-
One should suspect bullet embolism in a patient with a gunshot injury who presents an entry wound without an exit wound, even several years after the original incident.
-
Systematic physical examination, including cutaneous examination, is often the key to an aetiological hypothesis.
-
Owing to the paucity of these cases, no clear guidelines are available. Management must be individualised and discussed by a multidisciplinary team.
Footnotes
-
Contributors YY was involved in the conception, drafting and revision of the manuscript. DP was involved in the drafting and revision of the manuscript. AM was involved in the drafting and revision of the manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.