Article Text

Statistics from Altmetric.com
Description
A 6-year-old boy with frequent episodes of fever, myalgia and arthralgia, presented with arterial hypertension (HTN).
When he was 2 years old he was extensively investigated due to a small thalamic stroke, but no diagnosis was made.
While being evaluated for HTN, he presented with a medullar ischaemic stroke. Antinuclear and antineutrophil cytoplasmic antibodies were negative; there was no kidney failure, urinalysis changes or skin lesions. In the presence of recurrent fevers, ischaemic strokes and HTN, we suspected the presence of a vasculitis. A renal arteriography (figures 1 and 2) confirmed the diagnosis of childhood polyarteritis nodosa (cPAN), showing several microaneurysms and irregular constrictions in medium-sized and small-sized renal arteries.

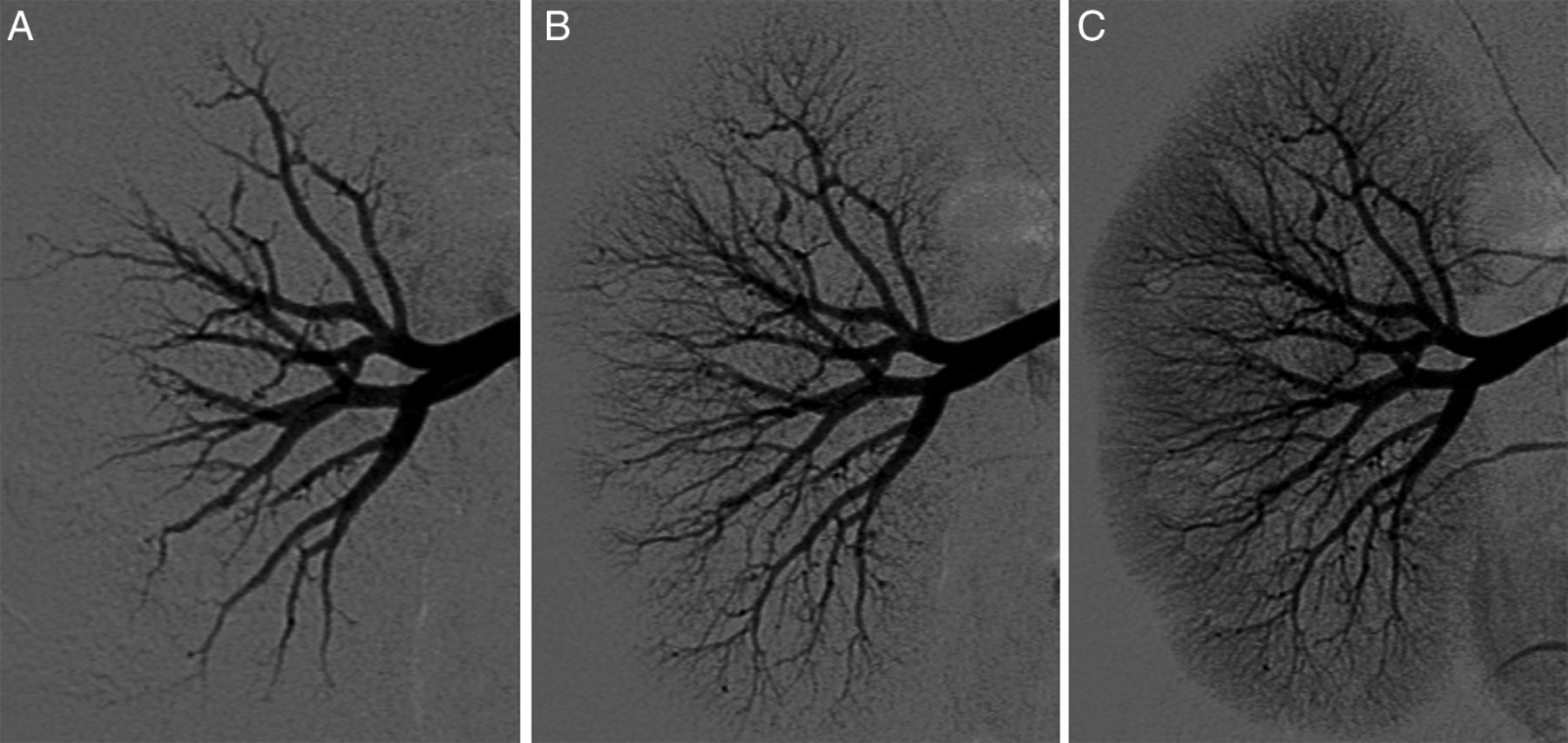
Right selective renal arteriography ((A–C) from early to late phase, respectively) showing several microaneurysms, segmental narrowing and variations in the calibre of arteries in medium-sized and small-sized renal arteries.

{kind=link}
{kind=link}
Left selective renal arteriography ((A–C) from early to late phase, respectively) showing several microaneurysms, segmental narrowing and variations in the calibre of arteries in medium-sized and small-sized renal arteries.
The patient was treated with corticosteroids, ramipril, hypocoagulation and monthly intravenous cyclophosphamide followed by azathioprine, and is currently asymptomatic, without significant deficits.
According to the EULAR/PReS classification criteria,1 the diagnosis of cPAN requires the mandatory presence of necrotising small-sized or medium-sized artery vasculitis or typical angiographical findings.
Several options are available for demonstrating renal involvement in cPAN,2 including less invasive techniques. MR angiography usually fails to detect microaneurysms and overestimates stenotic lesions.3 CT angiography performs similarly, at the expense of high ionising radiation exposure.3
Although biopsy is considered as gold standard for some territories, renal biopsy may fail to detect the pathognomonic changes due to sampling error.2 ,3 Also, the presence of small aneurysms increases the risk of bleeding or fistulae formation.2 ,3 Therefore, in cases such as this we advocate performing renal biopsy only in patients in whom the arteriography is negative.
Learning points
-
In addition to systemic symptoms, the presence of multiorgan involvement should heighten suspicion of vasculitis.
-
Vasculitis can present as ischaemic stroke at a young age.
-
Renal angiography is useful to confirm the diagnosis in patients with suspected childhood polyarteritis nodosa, particularly if the symptoms and laboratory abnormalities do not direct the choice of biopsy in other territories.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.