Article Text

Statistics from Altmetric.com
Description
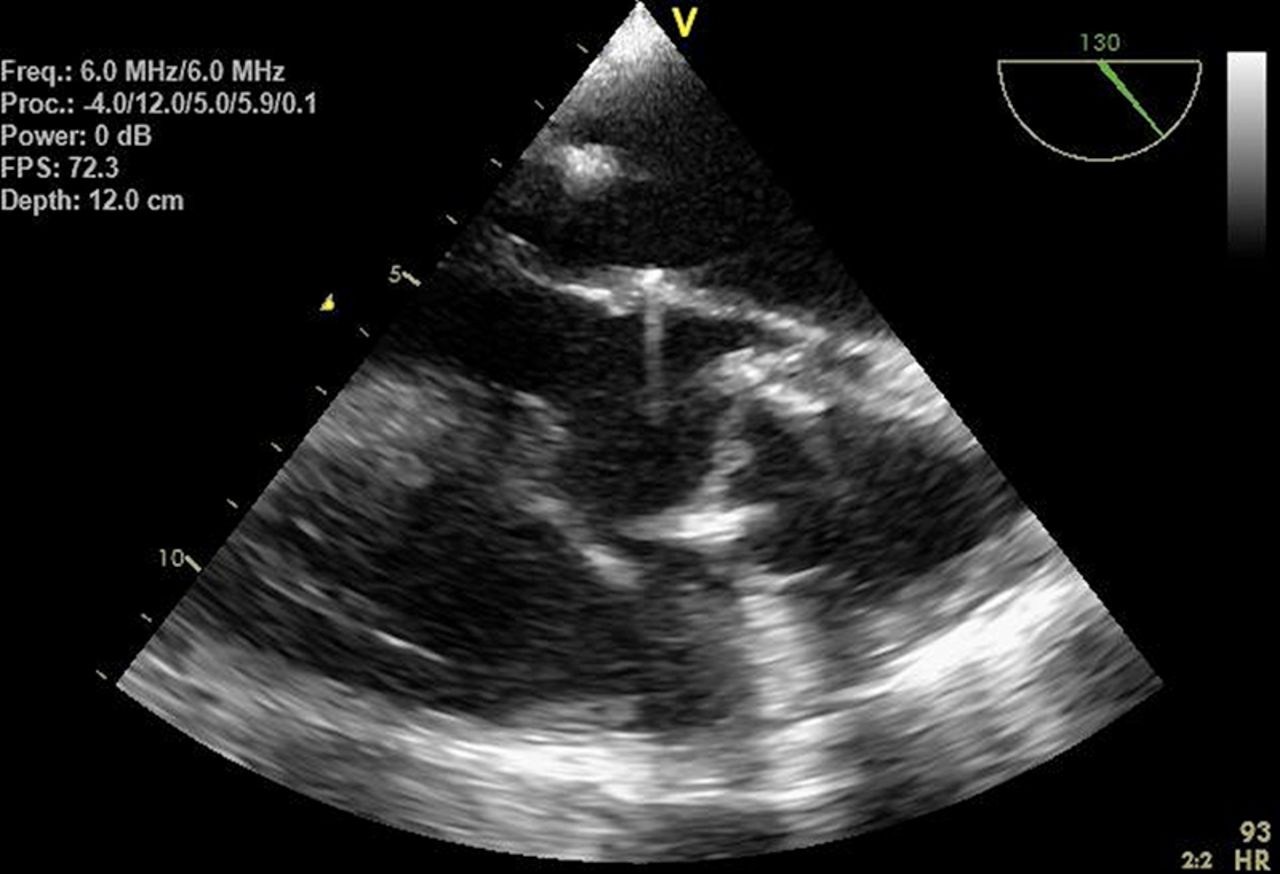
Images of a female patient's status post bioprosthetic aortic valve replacement with aortic root sparing and mitral valve repair. She presented with shortness of breath and low-grade fever 3 months after surgery. Transthoracic echocardiography (TTE) showed a freely mobile and rocking prosthetic aortic valve, totally dislodged and seeming to be stuck at the sinotubular level (figure 1), with a severe paravalvular leak causing aortic insufficiency (video 1). Holodiastolic flow reversal was observed in the descending thoracic aorta and normal left ventricular function. Transesophageal echocardiography (TEE) confirmed the findings (figure 2). The patient had positive blood cultures for coagulase-negative Staphylococcus and after an initial period of aggressive antibiotic therapy, she underwent minimally invasive aortic valve replacement re-do surgery (Bentall procedure) and made a gradual recovery (figure 3).

Transthoracic echocardiography apical view: dehisced and unseated bioprosthetic aortic valve.

Transesophageal echocardiography long axis: dehisced and unseated bioprosthetic aortic valve.

{kind=link}
{kind=link}
{kind=link}
Transthoracic echocardiography apical view: postoperative image of the newly placed bioprosthetic aortic valve.
TTE parasternal long axis (LAX): Dehisced and unseated bio-prosthetic aortic valve with severe paravalvular leak and aortic insufficiency.
The dehiscence of a prosthetic aortic valve is an uncommon complication that is reported in 0.1% to 1.3% of patients who undergo aortic valve replacement.1 The known risk factors for the dehiscence are bacterial endocarditis, concomitant aneurysm of the ascending aorta and severe calcification of the native aortic valve. Dehiscence of the aortic valve has also been noted with non-infectious aortitis and associated vasculitis.2 Total dislodgement with unseating of the bioprosthesis is very uncommon, hence we presented these striking images of this complication.
Learning points
Prosthetic valve endocarditis should be suspected with new murmur and fever in patients with a history of valve replacement.
Transesophageal echocardiography is helpful to confirm the diagnosis.
Complete dehiscence of a prosthetic valve is unusual but is commonly associated with infective endocarditis.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.