Article Text

Statistics from Altmetric.com
Description
A 55-year-old man presented with haematemesis on a background of 6 months of nausea, vomiting and 15 kg weight loss. He was clinically emaciated and dehydrated.
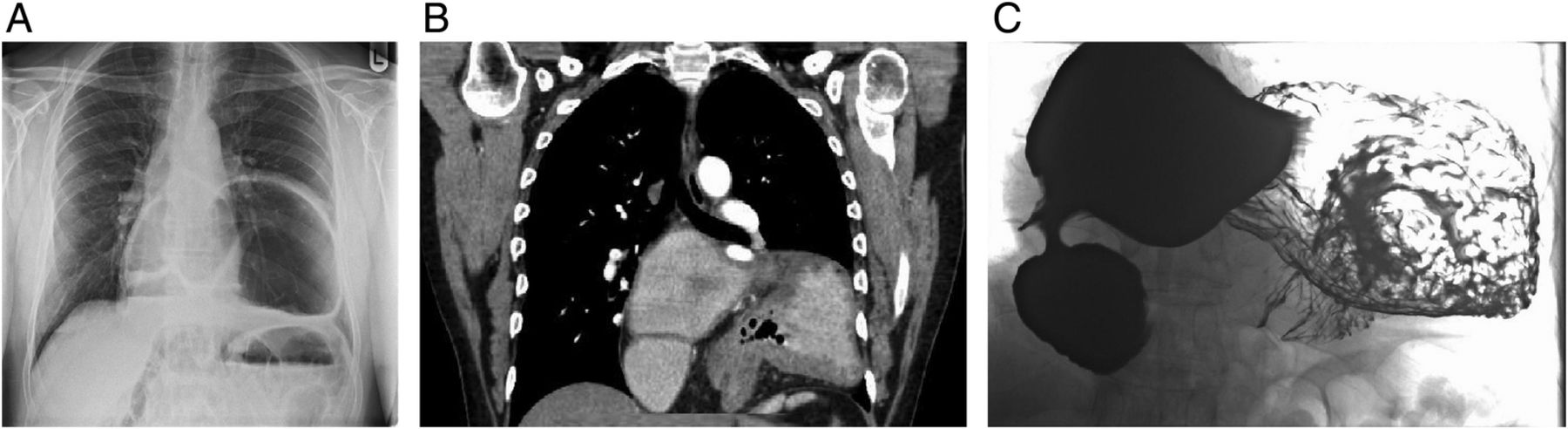
Chest X-ray demonstrated intrathoracic stomach with air–fluid levels within (figure 1A). Oesophagogastroscopy was performed, which demonstrated a large hiatus hernia with no evidence of bleeding. Follow-up CT and barium meal confirmed herniation of the entire stomach into the posterior mediastinum with associated mesenteroaxial volvulus (figure 1B, C).

(A) Erect chest X-ray demonstrating intrathoracic stomach with air–fluid levels. (B and C) Coronal CT image and barium meal demonstrating complete gastric herniation into posterior mediastinum with associated volvulus and outlet obstruction. Gastro-oesophageal junction and fundus of stomach (arrow) seen at the same level as the duodenal bulb (arrowhead).
The patient underwent successful laparoscopic reduction of volvulus and repair of diaphragmatic hernia.
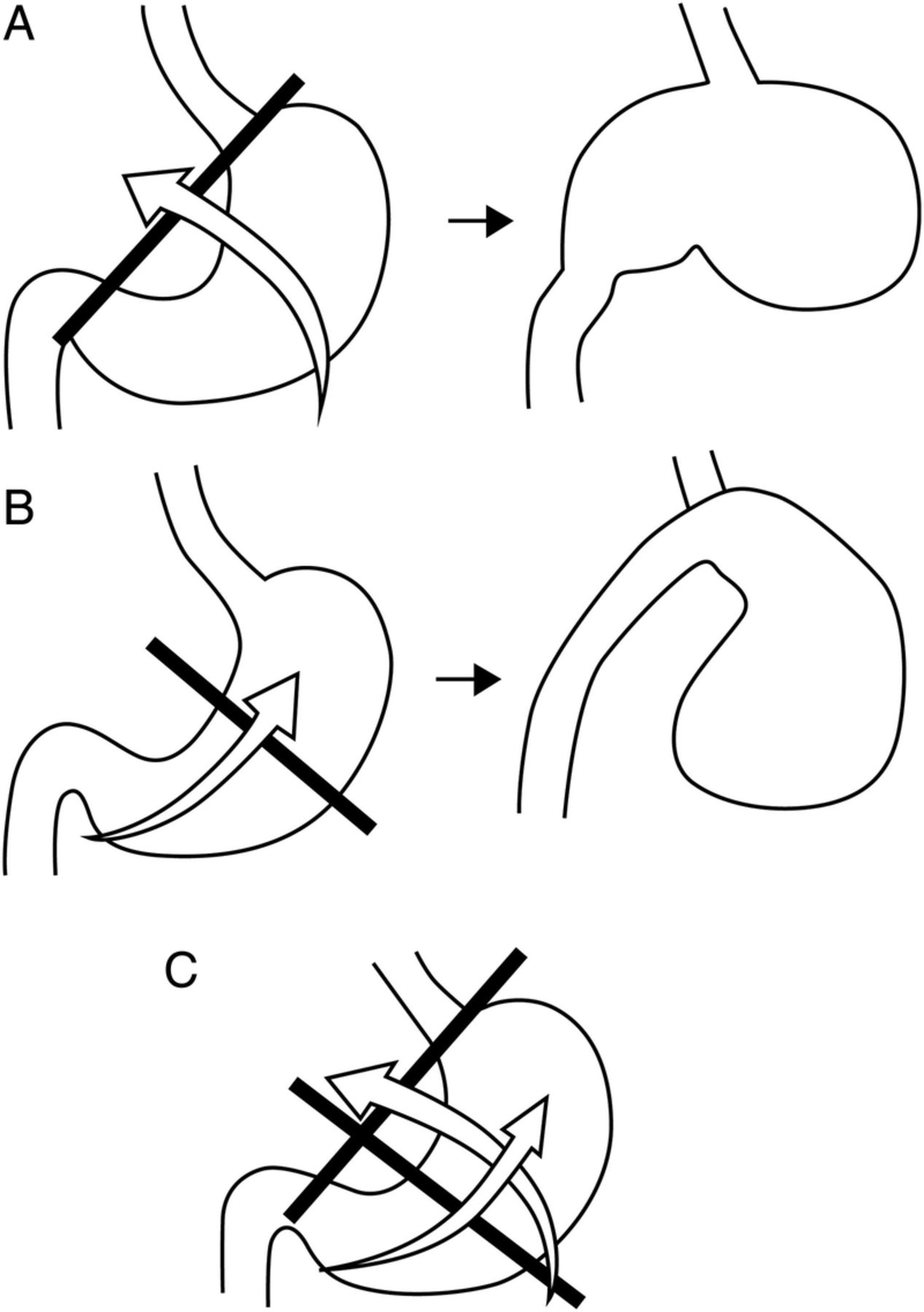
Gastric volvulus is defined as an acquired 180° rotation of the stomach creating a closed loop obstruction. It can present with gastric outlet obstruction, ischaemia and/or perforation.1 ,2 Borchardt’s triad of epigastralgia, retching and inability to pass a nasogastric tube are classical symptoms. Gastric volvulus can be classified into three types based on the axis of rotation (figure 2A, B, C). Organoaxial is the most common type and occurs when the stomach rotates along its long axis. Predisposing factors are a diaphragmatic defect or paraoesophageal hernia. Mesenteroaxial occurs when the stomach rotates around the transverse axis. Risk factors include abnormalities to gastric anchoring structures, for example, a long gastrohepatic ligament. The third type combines features of both. Ischaemia is more likely in mesenteroaxial and mixed types. Upper gastrointestinal tract contrast studies and CT are the imaging modalities of choice. Stable patients with no evidence of perforation can be managed laparoscopically with repair of hernial defect,3 while unstable patients require urgent open intervention.
Learning points
-
Gastric volvulus is defined as an acquired 180° rotation of the stomach creating a closed loop obstruction.
-
Gastric volvulus can be classified based on the axis of rotation into organoaxial, mesenteroaxial and mixed types.
-
Stable patients with no evidence of perforation can be successfully managed laparoscopically.

{kind=link}
{kind=link}
(A) Organoaxial volvulus (stomach rotates along its long axis). (B) Mesenteroaxial volvulus (the stomach rotates around the transgastric/short axis (a line connecting the middle of the lesser curvature with the middle of the greater curvature). (C) Mixed volvulus.
Footnotes
-
Contributors JMO prepared, researched and wrote the article, and DO supervised it. MM was involved in radiology opinion and editing courtesy and further editorial insight was provided by SR.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.