Article Text

Summary
The authors describe a seminal case report of a 10-year-old boy with enlarged gingivae in relation to his maxillary anterior teeth. The lesion, provisionally diagnosed as idiopathic gingival enlargement, was completely excised and divided into two sections. The histological and immunohistochemical findings in one of the sections showed it to be characteristic of schwannoma while the other section showed indications of idiopathic gingival enlargement. The patient has been followed up carefully and no recurrence has been noted.
Statistics from Altmetric.com
Background
Schwannoma is an uncommon intraoral benign neural sheath tumour which usually presents as a solitary encapsulated firm mass with a smooth surface. We present an unusual case with coalescence of diffuse gingival overgrowth and schwannoma which differed significantly from the usual presentation.
Case presentation
A 10-year-old boy presented to our department of periodontology with a six-month history of progressively increasing painless swelling of the gums in relation to the upper front teeth and an inability to form a lip seal. The patient was not taking any medication and his guardian reported no remarkable medical or family history. The patient reported that the swelling started with a localised freely movable growth in the upper left canine region which gradually became generalised and non-movable, involving a number of upper teeth. On clinical examination, a diffuse gingival overgrowth involving the marginal and attached labial gingiva was noted, extending from the right maxillary to the left maxillary canine. The gingiva was pink, non-erythematous and of firm consistency with loss of stippling. Bleeding on probing (BOP+), which was checked by running the probe in the sulcus area, was seen in 23.5% of the sites in the associated dentition (figure 1). The mean±SD plaque index and gingival index were 1.26±0.14 and 1.81±0.20, indicating fair oral hygiene, although stains were present palatally on the maxillary anterior teeth. Owing to the patient's age, medical history, clinical presentation and non-hereditary nature, a provisional diagnosis of idiopathic gingival enlargement was made.

Intraoral appearance of the diffuse gingival overgrowth extending from the left maxillary to the right maxillary canine.
Investigations
To rule out any bony involvement, a panoramic radiograph was advised which showed no abnormality including no signs of bone loss (figure 2). Routine haematological investigations conducted before the intervention were all within the reference range.

Preoperative panoramic radiograph showing unexceptional bone topography.
Differential diagnosis
Idiopathic gingival enlargement must be differentiated from chronic hyperplastic gingivitis and orofacial granulomatosis, whereas schwannoma must be differentiated from granular cell tumours, irritation fibromas, neurofibromas, leiomyomas, haemangiomas, lipomas, pyogenic granulomas, rhabdomyomas, benign salivary gland tumours, nerve sheath myxoma, palisaded encapsulated neurinoma, mucosal neurinoma associated with multiple endocrine neoplasias III and traumatic neuroma on the basis of hereditary pattern, history, clinical presentation and histological findings.
Treatment
A gingivectomy procedure was planned. Routine hematological investigations were carried out and the patient was prepared with thorough scaling and root planing. Oral hygiene instructions were instituted. We excised the enlarged tissue under block anaesthesia and the operated area was packed with a surgical periodontal dressing. The excised gingival tissue was cut into two small sections, which appeared pale pink and fibrous and did not differ from usual diffusely enlarged gingival tissue. The specimens (figure 3) were then sent for histopathological examination.

Gross appearance of the excised gingival tissue.
Outcome and follow-up
The patient returned after 10 days for pack removal. Healing had occurred uneventfully and the area appeared normal on the first recall visit (figure 4). Oral hygiene instructions were again reinforced. No recurrence was observed during follow-up. The patient also underwent a thorough physical examination to rule out the presence of multiple tumours. Patient satisfaction was evaluated by a targeted questionnaire and judged on the basis of a customised 3-point rating scale as described under section “Patient perspective” which showed that the patient was satisfied with the treatment outcome with a total (mean) of 2.66 (surgical procedure: 2; post-surgical phase: 3; cost-effectiveness. The recall examination showed no signs of recurrence. We were thus able to offer tangible benefits to the patient in terms of aesthetics, comfort and function.

Postoperative clinical appearance.
Discussion
Gingival overgrowth is characterised by progressive enlargement of the gingiva caused by an increase in submucosal connective tissue elements. Many cases are iatrogenic; some are inherited while others are idiopathic in nature.1 Although recent studies have associated idiopathic gingival overgrowth with changes in the SOS1 (son-of-sevenless 1) gene on chromosome 2 and have challenged the very existence of a true idiopathic gingival overgrowth,1 in the present case a provisional diagnosis of idiopathic gingival overgrowth was made due to the clinical presentation.
Schwannoma, also referred to as neurilemmoma, perineural fibroblastoma, neurinoma, lemmoma or Schwann cell tumour, is a rare benign neoplasm derived from the perineural Schwann cells.2 In 1910 Verocay gave the elementary description of this variety of tumour. Intriguingly, 25–48% of these otherwise infrequent lesions are located in the cervicofacial area,3 ,4 of which only 1% occur intraorally.5 Schwannoma may present at any age with no gender predilection, and the tongue seems to be the usual site for its occurrence intraorally with a proclivity towards the anterior segment; the order of propensity of occurrence is the palate, floor of the mouth, buccal mucosa, lip and the gingivae.6 ,7 Schwannomas originate as benign neural sheath tumours derived from the proliferation of Schwann cells. The head and neck regions have been found to be relatively common sites for the incidence of this tumour, as described by Ehrlich and Martin.2 However, schwannomas account for only 1% of benign tumours that occur in the oral cavity.5 With no pathognomonic features, the soft tissue lesion is generally a single circumscribed painless nodule of varying size which may simulate a large number of benign oral soft tissue lesions.
A tentative clinical diagnosis of schwannoma is difficult to establish, and identification of the lesion sometimes comes as a surprise.8 Sanchis et al,9 in a series of 12 cases of intraoral schwannoma, reported the initial diagnosis to be correct in only two cases while the other cases were tentatively diagnosed as fibroma, dermoid cyst, adenoma and even residual cyst. Although the clinical picture of the lesion at the time of presentation in our case differed from that shown classically by schwannoma, the history given by the patient of the presence of a nodule-like mass initially and gingival overgrowth might have masked the true character of the lesion which was revealed histopathologically. This is the first report of a schwannoma amalgamated with diffuse gingival enlargement.
Microscopic examination of H&E-stained tissue shows an encapsulated tumour consisting of two histological motifs that may be present in differing proportions. The most promptly recognised motif is the Antoni A tissue, which is composed of spindle-shaped cells arranged in a palisade fashion around acellular hyaline zones known as Verocay bodies. Antoni B tissue comprises erratically arranged spindle or oval cells in a myxoid background with microcystic changes. The histological findings of the present case were in agreement with this description, with a predominance of Antoni type A tissue pattern (figure 5). According to Chrysomali et al,10 tumour cells with Antoni A tissue have greater intensity scores than those with the Antoni B tumour pattern. These histological features distinguish schwannoma from neurofibroma (which lack the Antoni A and B pattern of schwannoma and are not encapsulated), perineurioma (which are S100 negative) and dermatofibromasarcoma protuberans (which are CD34 positive, lack S100 positivity and the Antoni A and B pattern of schwannoma).
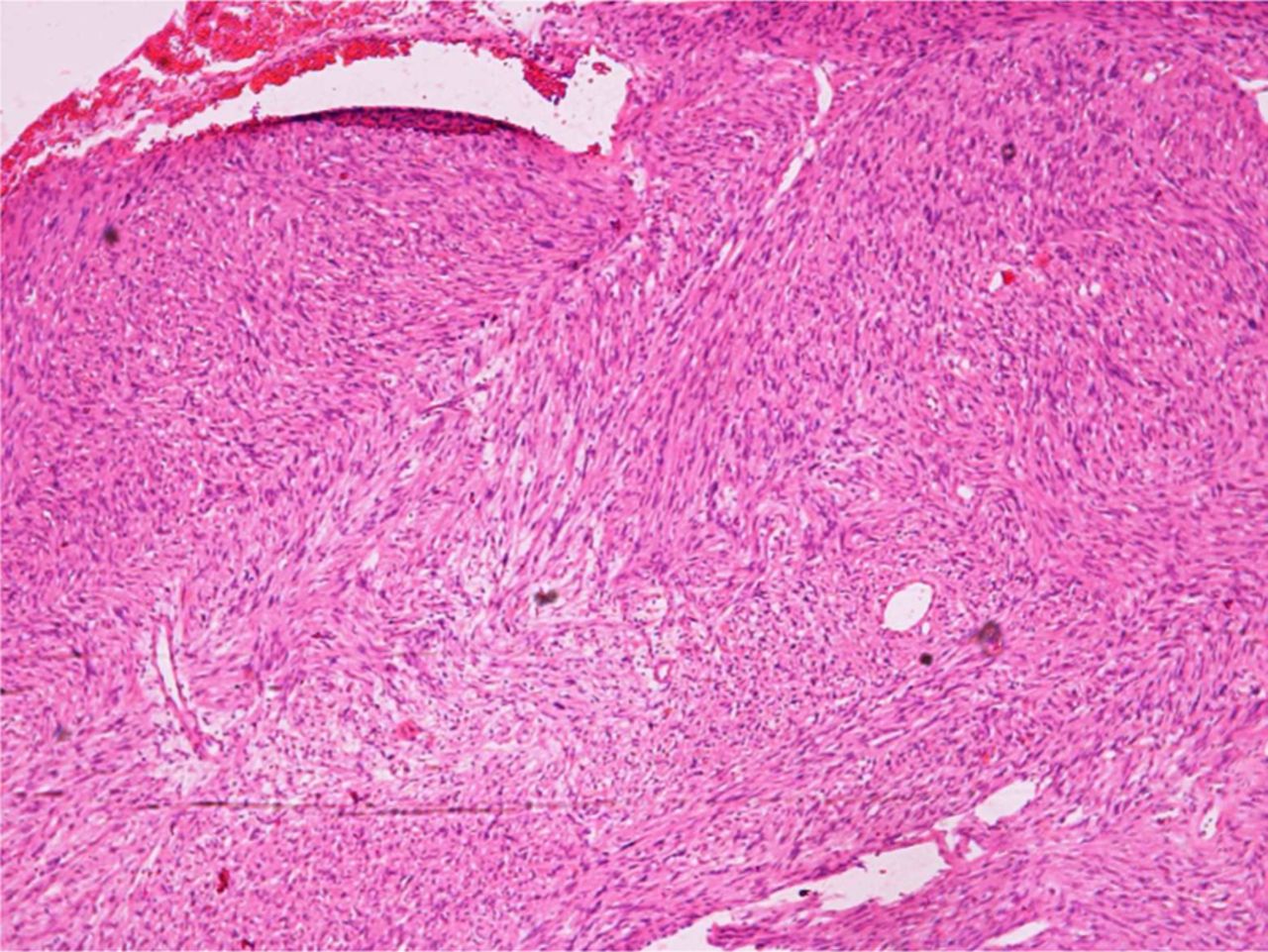
Photomicrograph of the lesion demonstrating characteristic Antoni A and Antoni B tissue patterns with a predominance of the former. Distinct hyalinised zones called Verocay bodies are also evident.
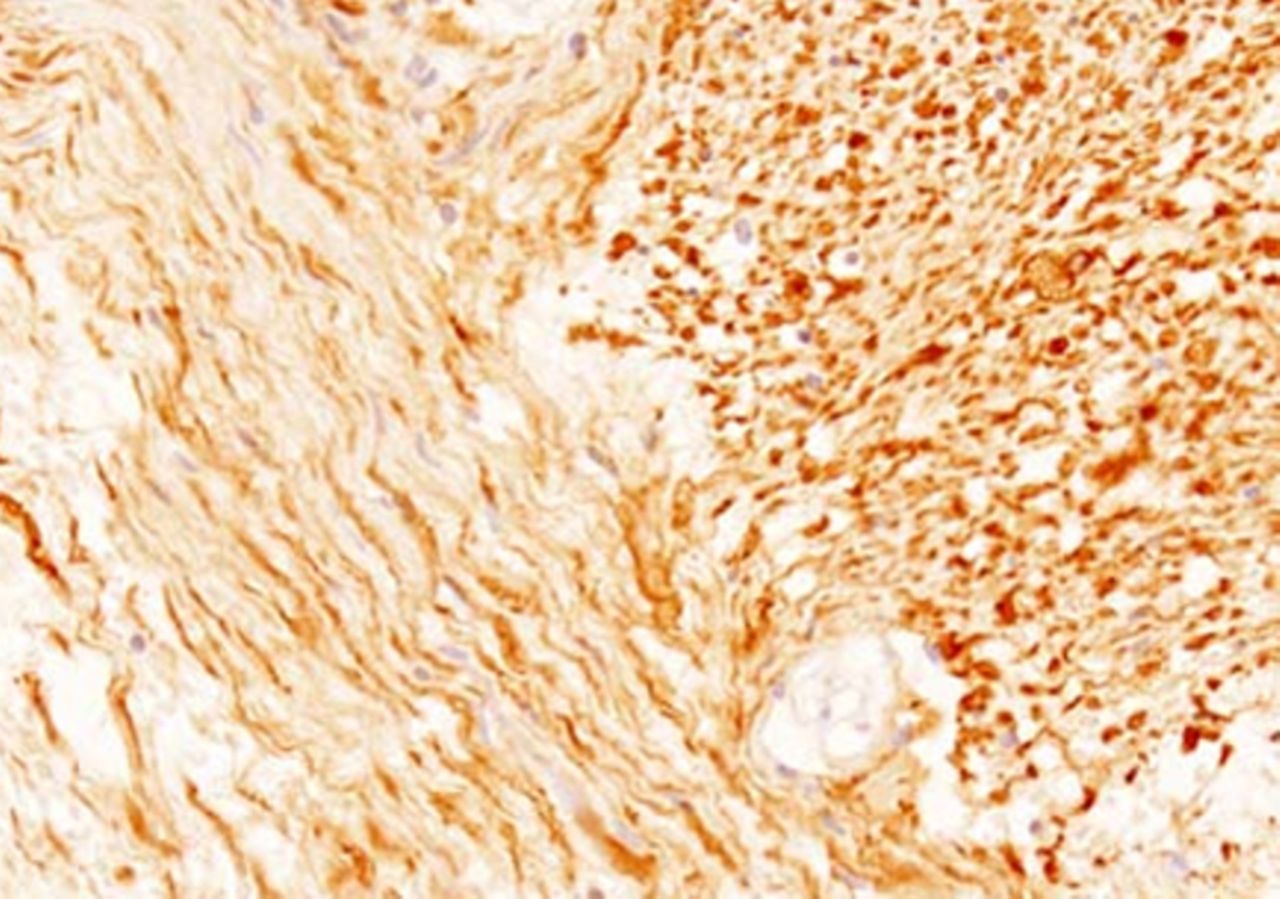
Considering the organisational pattern of tumoral Schwann cells forming Verocay bodies, immunohistochemical analysis for S100 protein was found to be likewise profoundly positive. S100 belongs to the family of calcium binding proteins such as calmodulin and troponin C. S100 staining was performed with avidin biotin complex which demonstrated tumour cells staining strongly positive for the S100 protein (a specific neural tissue marker; figure 6). The left side shows the Antoni B area which is more myxoid and vacuolated than the Antoni A area on the right side, which is more dense with the cells arranged in fascicles. These histological features distinguish the current lesion from neurofibromatosis and other S100 positive lesions including neurofibroma. However, in the second specimen a non-specific chronic inflammatory infiltrate was seen. Thus, histologically the lesion was an amalgamation of idiopathic gingival overgrowth and schwannoma.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
S100 positive slide showing Antoni B area on the left side which is more myxoid and vacuolated than the Antoni A area on the right, which is more dense with the cells arranged in fascicles.
Patients with neurilemmoma have a very good prognosis with almost no recurrence; however, exiguous recurrence has been noted with larger tumours with a broader extension. Partial removal may be necessary to prevent extensive sacrifice of vital structures such as an adjacent nerve. It is possible that the lesion discussed here may have arisen from the infraorbital nerve which innervates the concerned area.
Patient's perspective
-
The patient perspective was evaluated by means of a 3-point patient satisfaction rating scale where a score of 1 indicates that the patient is unsatisfied, a score of 2 indicates that the patient is satisfied and a score of 3 indicates that the patient is fully satisfied.
Learning points
-
General practitioners must be aware of such concealed lesions.
-
Referral to the relevant specialist is mandatory for appropriate diagnosis and management.
-
Schwannomas may present in a variety of forms and in combination with other pathological entities.
-
Schwannomas are usually asymptomatic and are detected accidentally.
-
Conservative surgical excision is the treatment of choice and the chances of recurrence are low.
Acknowledgments
The authors thank Dr Manish Singh, postgraduate student, Department of Pathology, AIIMS for his valuable support.
Footnotes
-
Contributors PP performed the surgical intervention; JD provided guidance for the entire case; KB assisted with surgery and the photography; SS assisted with the write-up and diagnosis.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.