Article Text

Statistics from Altmetric.com
Description
A 60-year-old woman, who was previously diagnosed with vasculitis on skin biopsy after developing maculopapular rash on lower extremities, presented with worsening dyspnoea, cough, blood-tinged sputum and night sweats. At emergency department , she was tachycardic and tachypneic with SpO2 of 86%. Arterial blood gas showed a pH of 7.45, pCO2 36 mm Hg, pO2 55.4 mm Hg, bicarbonate 25.0 mmol/L, SaO2 83.5%, and complete blood count revealed a white cell count of 24.9 K/μL and Hb 8.9 g/dL, which dropped down to 7.2 g/dL over the next 24 h (figure 1). Chest X-ray showed bilateral airspace opacities (figure 2) and the following CT scan demonstrated severe central pneumonitis consistent with alveolar haemorrhage (figure 3A,B). For respiratory failure, she was intubated, and bronchoscopic examination showed fresh blood in the right middle lobe without identified bleeding sites. Differential cell counts of bronchoalveolar lavage revealed eosinophils 11%, lymphocytes 9%, macrophages 30%, neutrophils 50% and red blood cells of 4530/μL with a negative infectious workup. Further examinations for autoimmune diseases were all negative except elevated perinuclear anti-neutrophil cytoplasmic antibodies (p-ANCA) and myeloperoxidase antibody, confirming the diagnosis of diffuse alveolar haemorrhage (DAH) associated with p-ANCA vasculitis.1

Laboratory values during the hospitalisation. The patient presented with elevated white cell count, haemoglobin and erythrocyte sedimentation rate suggesting active phase of vasculitis. Laboratory values were gradually normalised over the rituximab treatments.
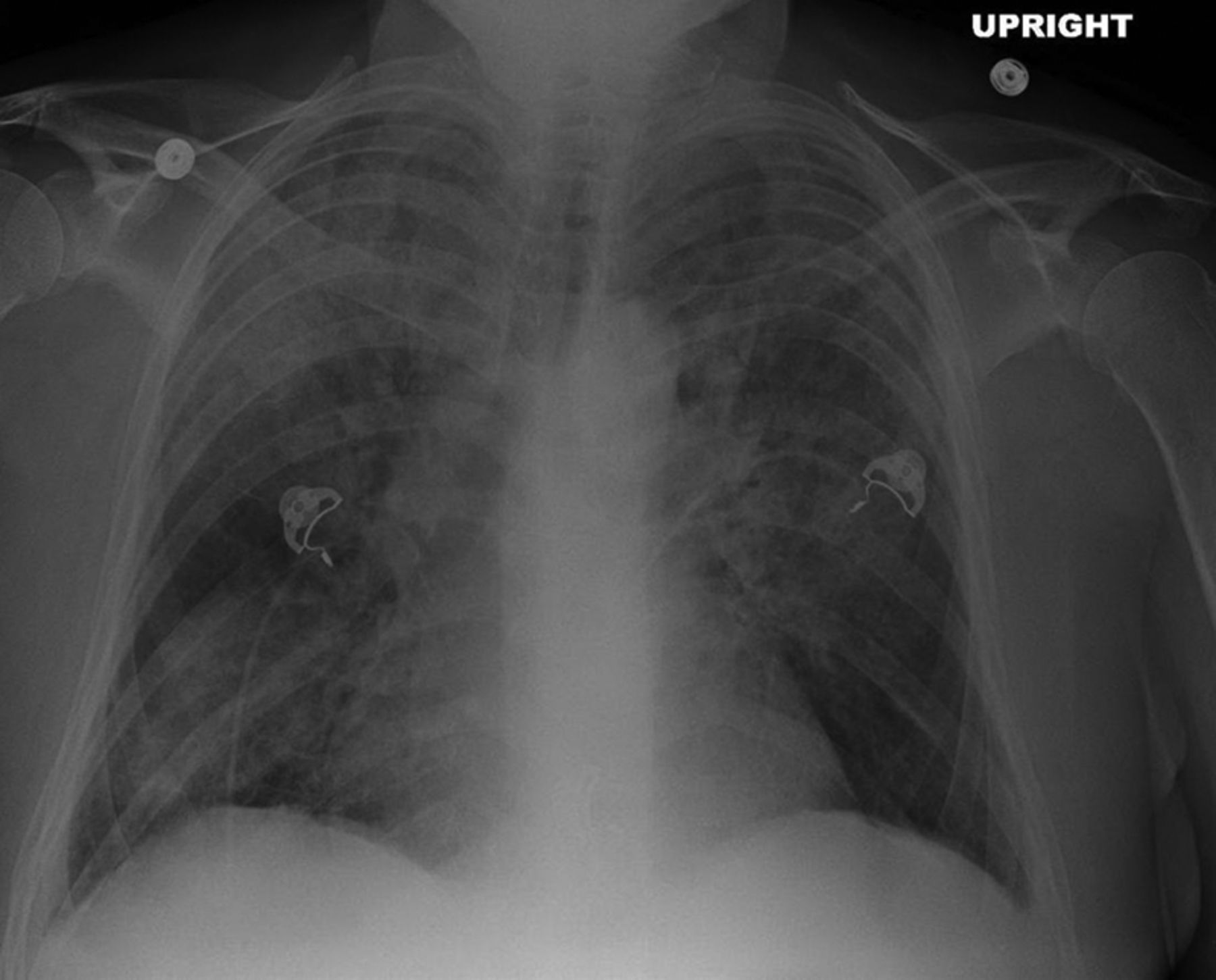
Chest X-ray anteroposterior view showing left upper lobe and right upper and lower lobe airspace disease without evidence of pneumothorax.

(A, B) CT chest with contrast shows severe bilateral symmetric and central pneumonitis consistent with haemorrhagic pneumonitis. Central airways are patent and clear. There is no evidence of pneumothorax, mediastinal, hilar or axillary lymphadenopathy. Bilateral pleural effusions are present.
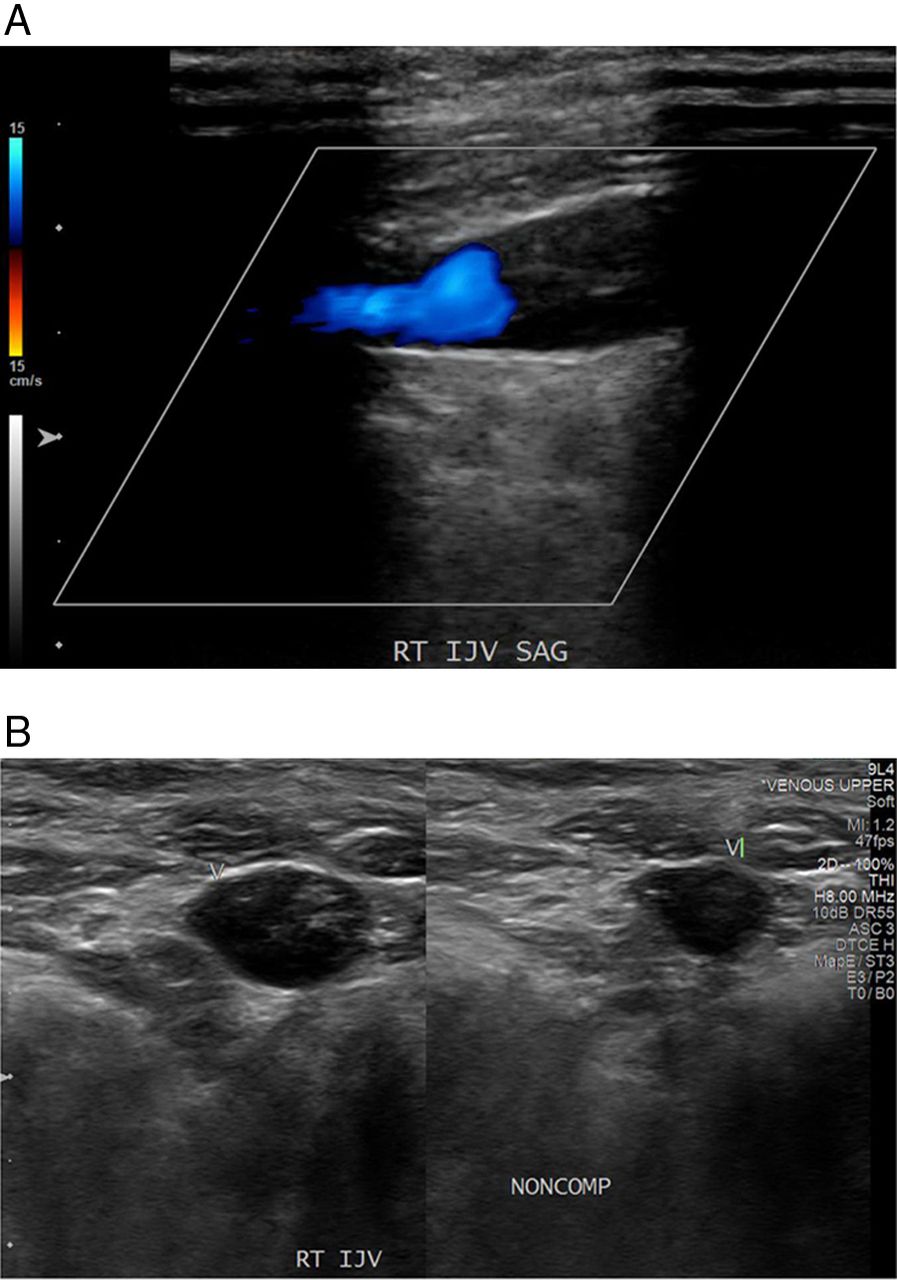
The patient achieved remarkable laboratory (figure 1) and clinical improvement (figure 4A,B) after high-dose steroid and 2 cycles of weekly rituximab treatment, and was successfully extubated. WBC and erythrocyte sedimentation rate (ESR) measured before extubation were 15.6 K/μL and 62 MM/HR, respectively, suggesting still active phase of vasculitis. Unfortunately, the patient developed another episode of respiratory failure requiring reintubation the next day. CT scan revealed new pulmonary embolism in the right upper lobe artery, and ultrasound demonstrated extensive thrombus in the right subclavian, axillary and internal jugular veins (figure 5). Owing to high risk of rebleeding, pharmacological anticoagulation was deferred until completion of total 4 cycles of rituximab treatment with normalisation of WBC and ESR, and the patient was discharged with warfarin without further complication.

(A, B) CT scan after high-dose steroid and rituximab treatment shows diffuse and airspace disease with some interstitial component in the mid and lower lungs. Superimposed areas of consolidation seen in figure 2 appear improved significantly, suggesting resolving diffuse alveolar haemorrhage.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A, B) Venous duplex ultrasound showing extensive deep vein thrombosis of the upper extremity with non-compressible occlusive thrombus in the right internal jugular, subclavian and axillary veins.
Pulmonary manifestation of p-ANCA associated vasculitis includes cough, haemoptysis and dyspnoea. In the systemic involvement of vasculitis, it can progress to life-threatening diffuse alveolar haemorrhage (DAH) with respiratory and cardiovascular decompensation.2 ,3 Paradoxically, p-ANCA associated vasculitis is also known as a high-risk factor for venous thromboembolism (VTE) and the majority of VTE cases develop during the active phase of vasculitis.4 ,5 Treating concurrent DAH and VTE in active disease is very challenging. Anticoagulation can be started with careful monitoring once active vasculitis is controlled with a single or combination regimen of steroid, anti-tumour necrosis factor-α (anti-TNF-α) and rituximab as described in this case.
Learning points
-
Lung disease of perinuclear anti-neutrophil cytoplasmic antibodies (p-ANCA) associated vasculitis presents with respiratory symptoms including haemoptysis and dyspnoea, and it can progress to life-threatening alveolar haemorrhage.
-
ANCA associated vasculitis is one of the high-risk factors for venous thromboembolism, which develops during the active phase of vasculitis in the majority of cases.
-
Pharmacological anticoagulation is contraindicated in active bleeding, and the mainstream of treatment is steroid, anti-tumour necrosis factor-α or rituximab in active disease.
Footnotes
-
Contributors SY, LH, SA and KJ were involved in the care of the patient, collecting data and all of the authors wrote the case report. SY reviewed the literature and revised the manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.