Article Text

Summary
Facial and cervical area sinus tracts can be odontogenic or non-odontogenic, and so clinicians should be aware that lesions with a dental origin can be confused with dermatological lesions. We describe three cases of cutaneous lesions of dental origin that were initially misdiagnosed as being dermatological in origin. Multiple unsuccessful treatments were attempted but the lesions failed to heal. However, conservative endodontic intervention resulted in complete resolution of the causative periapical lesions within a short period, making surgery unnecessary. Dental aetiology, as part of a differential diagnosis, must be considered in such oro-facial lesions.
Statistics from Altmetric.com
Background
When a draining lesion is encountered in the facial area, a dental aetiology should always be considered for a correct diagnosis. Non-surgical conservative endodontic therapy, possibly followed by endodontic surgery or extraction, is the treatment of choice for these cases without the need for plastic or laser surgery.
Case presentation
Introduction
Chronic inflammation of pulpal origin is one cause of cutaneous sinus tract in the facial region, which is rare compared to an intra-oral sinus and may result from a longstanding inflammatory process associated with necrotic pulp.1 ,2 Patients are usually healthy and unaware of the associated dental problem, thus delaying the correct diagnosis and treatment of extra-oral sinus lesions with a primary odontogenic origin.3 Approximately 50% of patients undergo multiple surgical interventions and/or biopsies, are given repeated courses of antimicrobials, and even undergo radiation therapy or electrodessication before the correct diagnosis is made.4 ,5
The cases described here presented with a persistent cutaneous sinus tract of dental origin that was misdiagnosed by a general physician but which showed complete resolution following dental treatment.
Case reports
Case 1
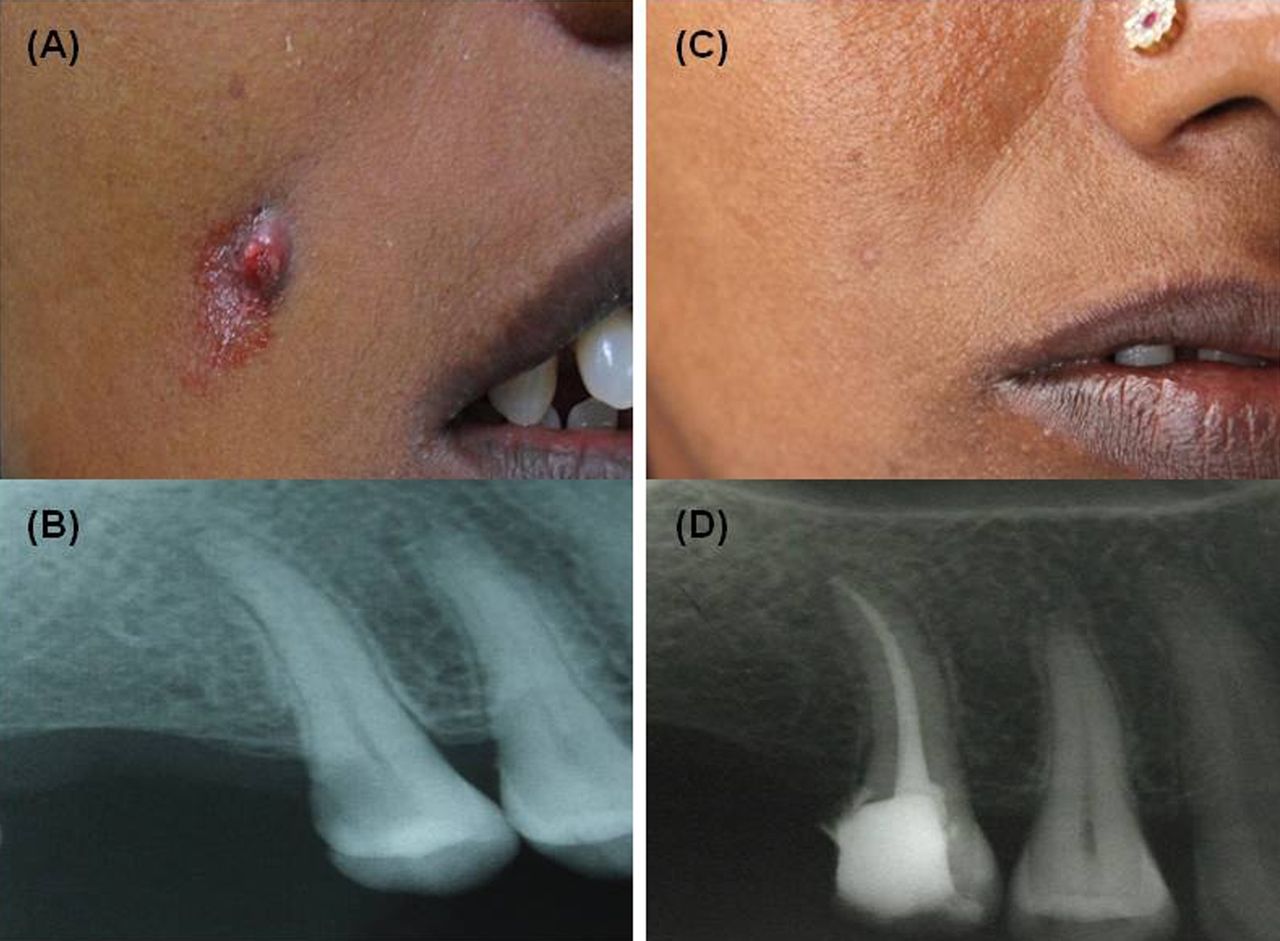
A 23-year-old female patient reported to our department with a chief complaint of a facial lesion on the right side in the zygomatic region. The patient had a 1-month history of recurrence and remission of fever, for which she had been treated by a medical practitioner. Since there was repeated occurrence of the lesion, she was referred to our dental institute for an opinion. On the day of examination, the patient was afebrile and had no systemic disease. Extra-oral examination revealed an erythematous nodule with continuous drainage on the right side of the cheek (figure 1A). The nodule was soft on palpation, which elicited a purulent discharge. The lesion had alternately appeared and disappeared over the previous 3 months. An intra-oral periapical X-ray (IOPA X-ray) examination revealed a maxillary second premolar that was cariously exposed (figure 1B). Endodontic treatment was initiated and an intra-canal dressing of calcium hydroxide was applied for 1 week. The extra-oral lesion resolved within 14 days after which the endodontic treatment was completed (figure 1C). Follow-up for 6 months showed symptomless and uneventful healing of the lesion as confirmed by a second intra-oral IOPA X-ray taken after 6 months (figure 1D).

(A) Pre-treatment photograph. (B) Pre-treatment radiograph. (C) Photograph 2 weeks after treatment. (D) Radiograph 6 months after treatment.
Case 2
A 12-year-old girl was referred from an oral and maxillofacial surgery department with a complaint of episodic drainage from a cutaneous lesion in the submental region. The medical history was not relevant. The lesion was approximately 2 cm in diameter (figure 2A). Exudate was seen after palpation and no vestibular swelling was present. Intra-oral examination revealed incomplete previous treatment of a mandibular left incisor. An intra-oral periapical radiograph showed radiolucency surrounding the mandibular left central incisors (figure 2B). A diagnosis of suppurative apical periodontitis of the responsible tooth was made with a requirement for root canal treatment. Root canal treatment was re-initiated, calcium hydroxide was inserted into the canal after root canal preparation, and the patient was recalled after a week. The extra-oral lesion resolved after 2 weeks (figure 2C), endodontic treatment was completed and final restoration was carried out with a light cured composite. The patient was recalled after 6 weeks, by which time the draining lesion had completely healed (figure 2D).

(A) Pre-treatment photograph. (B) Pre-treatment radiograph. (C) Photograph 2 weeks after treatment. (D) Radiograph 6 weeks after treatment.
Case 3
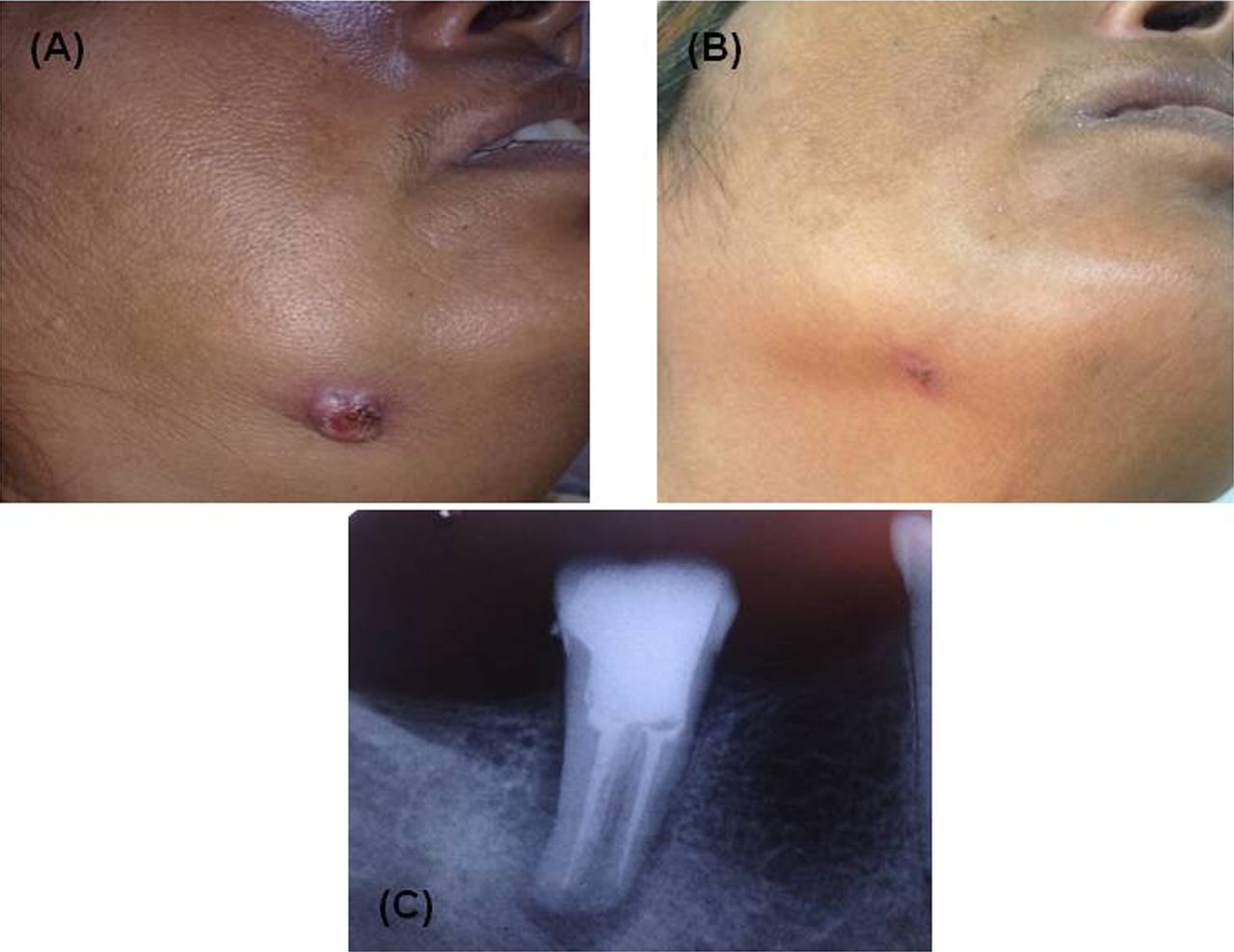
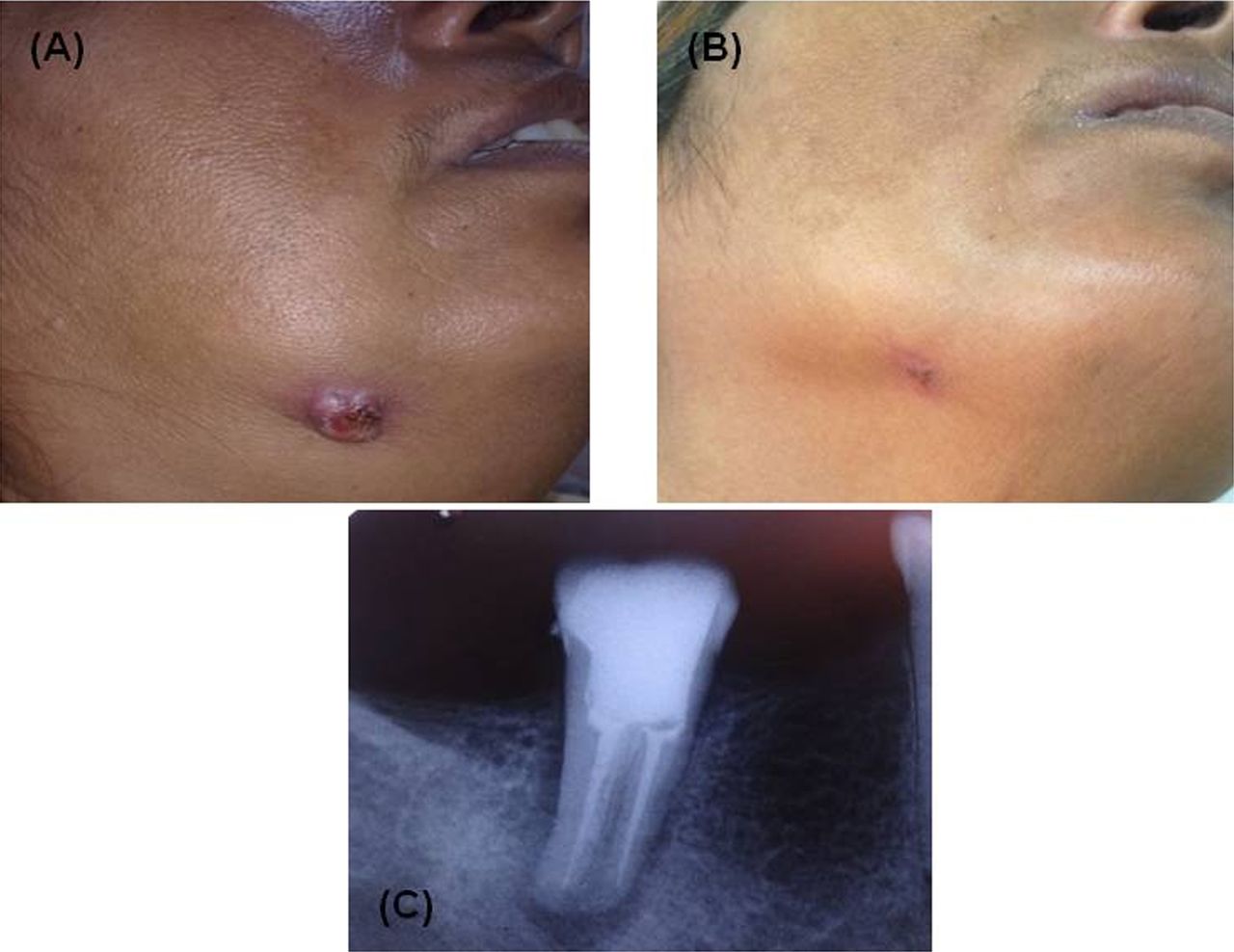
A 47-year-old woman presented with a nodular lesion on the lower border of the mandible that had been discharging pus intermittently for 7 months (figure 3A). She could not recall any previous trauma to the site. Dermatological examination revealed a non-tender, erythematous, nodular, draining lesion on right side of the face for which she had been repeatedly treated with antibiotics for 6 months. When the lesion did not resolve, the patient was referred for a dental opinion. Dental examination showed poor oral hygiene and severe chronic periodontitis, but no acute infection. An intra-oral radiograph demonstrated diffuse periapical radiolucency associated with the right mandibular second molar area. The patient was diagnosed with chronic apical periodontitis. Endodontic treatment was initiated and the working length of tooth determined using an apex locator. Irrigation of the root canal with saline resulted in the irrigant squirting out of the lesion, which confirmed that the lesion had an odontogenic origin. Chlorhexidine was preferred as an irrigant during the instrumentation procedure and was left in the canal for 10 min to ensure complete disinfection. The canal was dried and obturation carried out by the lateral condensation method. The extra-oral lesion resolved in 2 weeks (figure 3B) and the lesion healed within the 6-month follow-up period (figure 3C).
{kind=link}
{kind=link}
{kind=link}
(A) Pre-treatment photograph. (B) Photograph 2 weeks after treatment. (C) Radiograph 6 months after treatment.
Differential diagnosis
The differential diagnosis includes actinomycosis, pyogenic granuloma, dacryocystitis, furuncle, congenital fistulae, bisphosphonate-associated osteonecrosis, and various neoplastic diseases.
Treatment
Non-surgical endodontic therapy only was carried out.
Outcome and follow-up
Endodontic treatment provided complete healing of the periapical lesions in a short follow-up period of 6 weeks.
Discussion
Cutaneous sinus tract in the facial and cervical area can develop as result of dental pulpal necrosis and chronic periapical periodontitis. Possible dental causes include trauma, retained roots, residual chronic infection of the pulp, and jaw diseases.6 ,7 The purulent exudates of odontogenic infection will take the easiest path in the periapical area and the sinus tract exits as an intra-oral or extra-oral lesion depending on the location of muscle attachments and facial sheaths once the cortical plate has been penetrated.8 If the apices of the maxillary teeth are above the maxillary muscle attachments, or below for the mandibular teeth, the spread of infection may be extra-oral. Most cutaneous sinus tracts are associated with the anterior mandibular teeth, and these tracts arise in the chin or submental area of the face, while other common areas are the angle of the mandible and the naso-labial fold.9
For a physician, diagnosing cutaneous odontogenic sinuses can be challenging. Patients are often unaware that they have any dental problems, and the associated cutaneous lesion may appear early or up to 30 years after a primary dental problem has occurred. Also, the cutaneous lesion is often distant from the site of primary infection.10 Chronic purulent drainage through the sinus tract prevents pressure build-up, swelling and pain, and so most patients are asymptomatic. In addition, unsuspecting physicians often overlook the possibility that a dental infection may produce a draining sinus tract. A literature review revealed one case of cutaneous odontogenic sinus tract in which the correct diagnosis was made 32 years after the discharging lesion was first observed.11 ,12 As several non-odontogenic disorders may also produce a cutaneous sinus, the differential diagnosis is important for facilitating accurate clinical care. The differential diagnoses for this condition include infectious disease like actinomycosis, pyogenic granuloma, dacryocystitis, furuncle, congenital fistulae, bisphosphonate-associated osteonecrosis, and various neoplastic diseases.
Pyogenic granuloma is an inflammatory growth of soft tissue in the oral cavity, predominantly occurring in the second decade of life in young females. Clinically, pyogenic granuloma is a smooth, lobulated, exophytic lesion manifesting as a small, red, erythematous papule on a pedunculated or sessile base which is haemorrhagic. The surface colour ranges from pink to red to purple depending on the age of the lesion.
Cervicofacial actinomycosis is the most common clinical form of actinomycosis, which is a rare disease. There is a slight male prevalence in young adults. This bacterial infection is rare and diagnosis is difficult. Most cases of cervical actinomycosis are odontogenic in origin and occur predominantly in immune-competent individuals. Actinomyces are usually of low pathogenicity and cause disease only in the setting of previous tissue injury.
A group of highly diverse malignancies can affect organs and tissues of the oral cavity, for example, malignant lymphoma (the generic term given to tumours of the lymphoid system). This tumour can be divided into two main categories: Hodgkin’s lymphoma and non-Hodgkin’s lymphoma (NHL). Malignant lymphoma can appear in all parts of the body, with the head and neck being the second most common region for extra nodal lymphoma after the gastro-intestinal tract. NHL commonly involves oropharyngeal lymphoid tissue comprising Waldeyer’s ring, but occasionally affects other oral tissues as well. In children, NHL occurs more frequently in the head and neck region. Clinical signs and symptoms of lymphomas of the para-nasal sinuses include a mass in the nasal cavity, facial pain, paresthesia, recurrent sinusitis, nasal discharge, eyelid swelling, and proptosis if orbital invasion has occurred.
Bisphosphonate-associated osteonecrosis (BON) is a serious oral complication of bisphosphonate treatment, involving exposure of necrotic maxillary or mandibular bone. Bisphosphonates are used in the treatment of osteopenic disorders as they have a high binding affinity with bone and interfere with osteoclast function, thereby slowing bone remodelling and turnover. In paediatric patients, intravenous bisphosphonates are used in the management of osteogenesis imperfecta, idiopathic juvenile osteoporosis, and osteopenic patients with juvenile rheumatoid arthritis who receive large doses of corticosteroids or methotrexate. However, unlike the situation in adults, BON is thought to occur rarely, if at all, in children. In patients at risk of BON, osteomyelitis and osteonecrosis may occur following dental procedures. Common associated orofacial findings are poor wound healing, spontaneous or postsurgical soft-tissue breakdown leading to intra-oral or extra-oral bone exposure, bone necrosis, and osteomyelitis.13––15
Recognition of the cutaneous lesion as a sinus tract is the first important diagnostic step. Palpation of the involved area for a cord-like tract, and ‘milking’ this tract for purulent material can be helpful. After a detailed dental examination, including vitality tests, has been completed, the patient should undergo panoramic and periapical radiographic examination, and then a final diagnosis should made to allow for a definite treatment plan.13
Previously sinus tracts were thought to be lined with epithelium and therefore to need surgical intervention in addition to endodontic treatment. However, later studies suggested such tracts were lined with granulation tissue only and so could be treated by a non-surgical endodontic method.16 Non-surgical endodontic treatment using a calcium hydroxide dressing between appointments or surgical root canal therapy are the best options if the tooth can be restored. Due to its biological properties as a result of the dissociation in Ca2+ and OH− ion, calcium hydroxide is considered the best substance to induce hard tissue deposition and promote healing of vital pulpal and periapical tissue. The high pH and the ionic activity trigger the healing process in root canal and periapical infection. If this treatment is not possible, extraction of the tooth is indicated.17 Systemic antimicrobial therapy is neither necessary nor recommended, as it has only a temporary effect. Local excision of the lesion will not stop the drainage either, may cause tissue breakdown resulting in further facial deformity, and therefore should also be avoided. When appropriate dental treatment is carried out, drainage will cease and the sinus tract will spontaneously close within a few weeks.18
Learning points
-
An endodontic origin should always be considered for a facial lesion so correct diagnosis can be made and a definitive treatment plan instituted.
-
Conservative endodontic treatment, sometimes followed by periapical surgery or extraction, is the treatment of choice for such cases.
-
The presented case report describes non-surgical conservative endodontic management which resulted in the elimination of a cutaneous sinus tract of dental origin in patients with a good host response.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.