Article Text

Statistics from Altmetric.com
Description
A 30-year-old woman presented to our hospital with reports of dyspnoea on exertion with no prior history of cardiac illness. General examination revealed tachycardia, tachypnoea and a blood pressure difference between the upper and lower limbs with higher values in lower limbs. On systemic examination, apical impulse was localised in the fifth intercostal space medial to the midclavicular line and a grade 3/6 early diastolic murmur at the left parasternal region was noted. No peripheral signs of aortic regurgitation were present. ECG was within the normal limits. Echocardiogram performed revealed quadricuspid aortic valve (QAV) on parasternal short axis view (figures 1 and 2 and video 1). Doppler echocardiography showed central jet of aortic regurgitation (figure 3) and severity of aortic regurgitation calculated by pressure half-time method showed to be 510 ms suggestive of mild aortic regurgitation (figure 4). A normal aortic valve has three equal cusps. Abnormal cusps may be formed as a developmental anomaly. Bicuspid aortic valve is the most common anomaly of this kind with unicuspid valve being the second most common.1 Quadricuspid aortic valve is a very rare cardiac anomaly with incidence of 0.013–0.043%.2 Previously when echocardiography was not available most of the diagnosis of QAV was performed during the time of aortic valve surgery or autopsy.3 Hurwitz and Roberts4 categorised QAV into seven subtypes. Our patient had type A variety with four equal cusps, which is the second most common after type B which has three equal cusps and one small cusp being the most common type. The importance of recognising this condition lies in the fact that more than 50% of the people with QAV require valve replacement in the fifth or sixth decade of life, because of worsening aortic regurgitation. Hence, patients with diagnosis of QAV have to be under regular follow-up and planned for aortic valve replacement before left ventricle decompensation. QAV is a rare cause for isolated aortic regurgitation in young people where if diagnosis is not established by transthoracic echocardiography, transoesophageal echocardiography has to be performed to rule out the diagnosis. Except for aortic regurgitation, other abnormalities like hypertrophic cardiomyopathy,5 mitral valve prolapse6 and sinus of Valsalva7 were not seen in our patient. Our patient remained asymptomatic on follow-up on medical therapy for 10 years.

Parasternal short axis view showing quadricuspid aortic valve in systole.

Parasternal short axis view showing quadricuspid aortic valve in diastole.
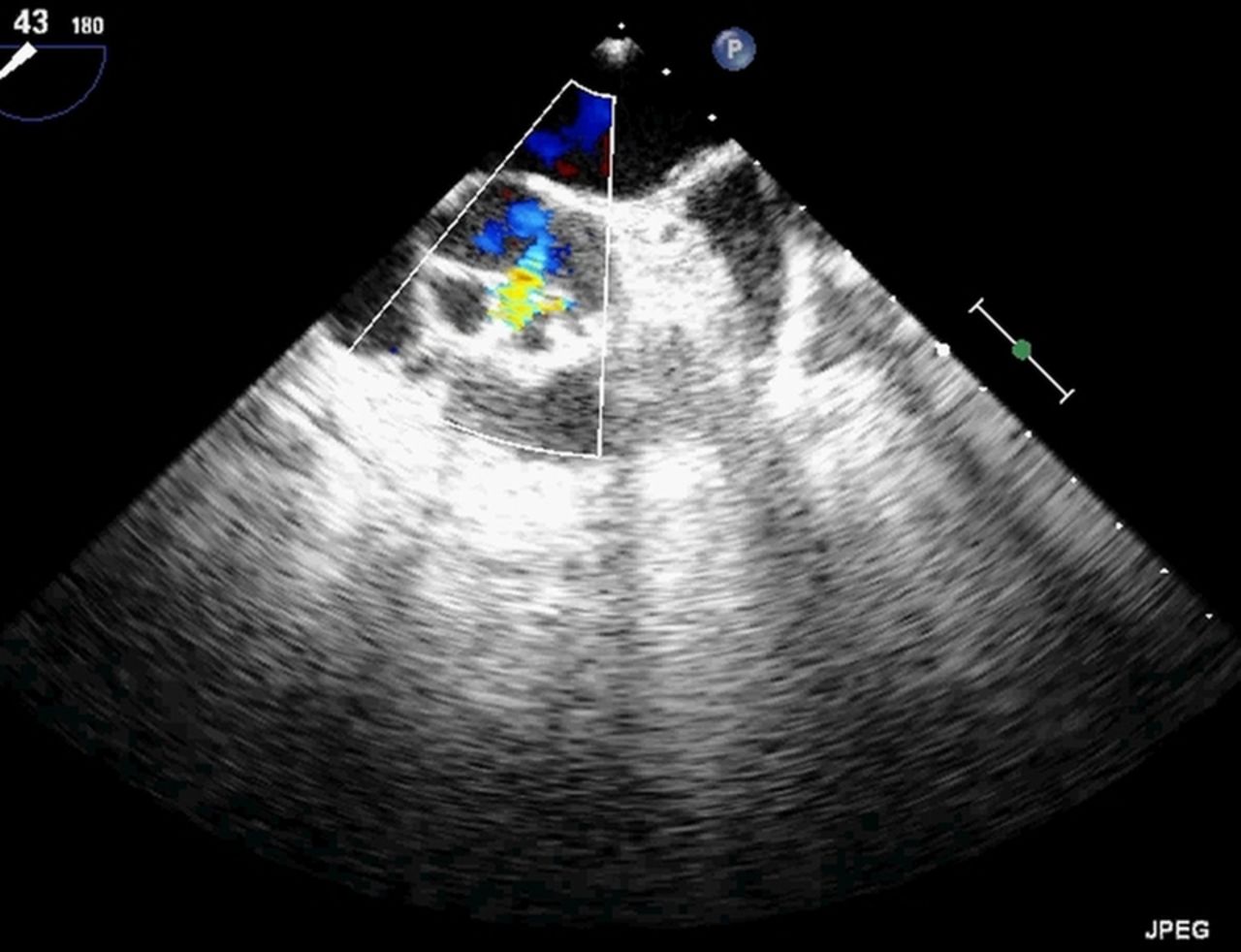
Parasternal short axis view Doppler mode showing central jet of aortic regurgitation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Continuous wave Doppler showing mild aortic regurgitation calculated by pressure half-time method.
Echocardiography short axis parasternal view showing quadricuspid aortic valve.
Learning points
-
Quadricuspid aortic valve (QAV) is a rare cause of aortic regurgitation.
-
Patients with QAV should be kept on regular follow-up as most of them require aortic valve replacement in the fifth or sixth decade in view of worsening aortic regurgitation.
-
Diagnosis of QAV should exclude associated conditions like hypertrophic cardiomyopathy, mitral valve prolapse and sinus of Valsalva.
Footnotes
-
Acknowledgements The authors thank Dr Padma kumar MD, DM Professor and Head of Cardiology, Kasturba Hospital, Manipal.
-
Contributors Drafting of the template and review of the literature was done by RRP and NM. Review before the final submission was done by HK and TD.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.