Article Text

Statistics from Altmetric.com
Description
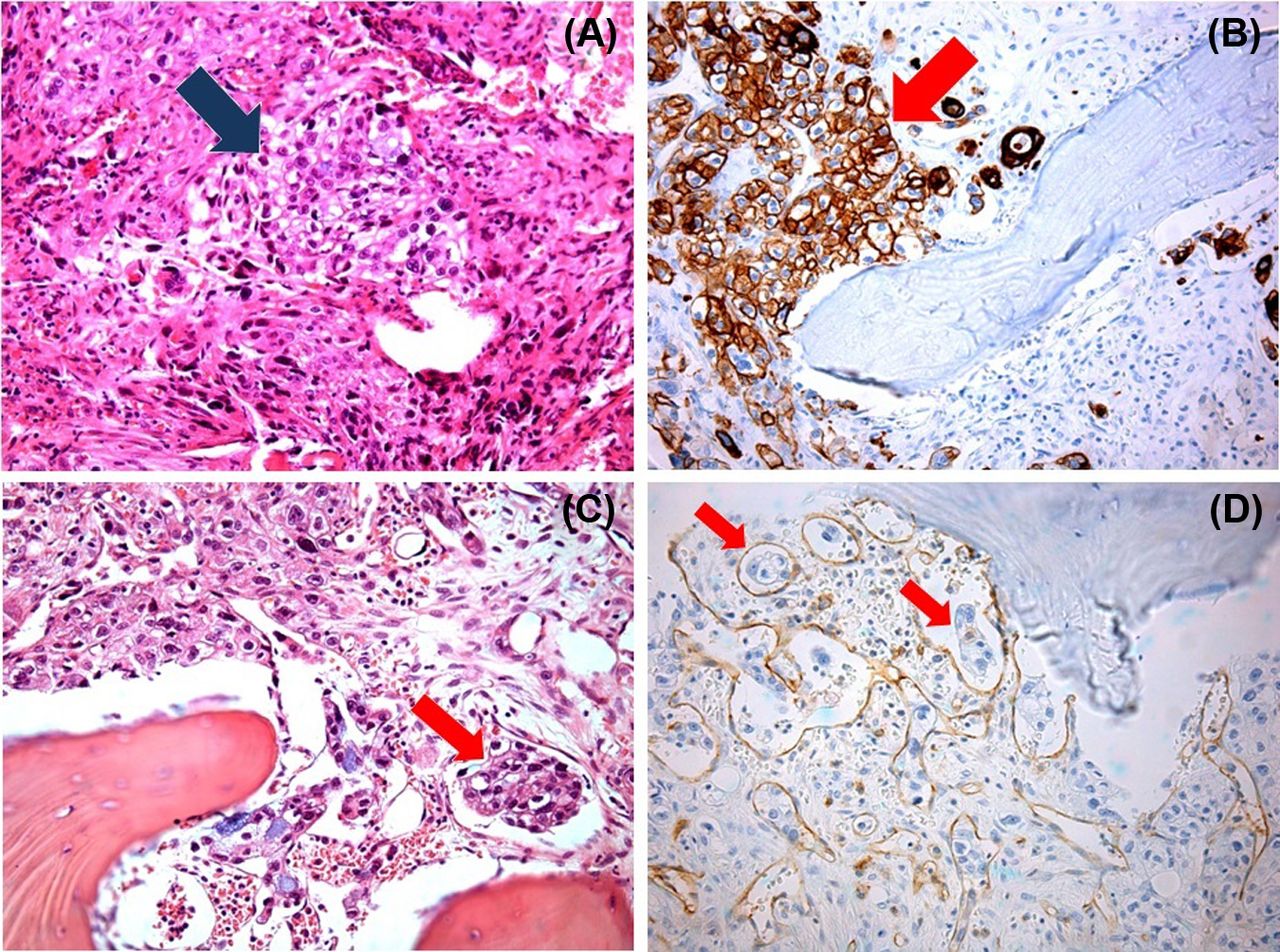
The authors illustrate the case report of a previously healthy, 50-year-old man with severe anaemia and thrombocytopenia, refractory to transfusional support, who was admitted in their hospital for the diagnostic investigation of multiple osteoblastic lesions in the lumbar vertebrae. Along with other complementary diagnostic examinations, upper endoscopy was performed identifying a gastric ulcer at the cardia level. Histopathology revealed a poor differentiated metastatic carcinoma with signet ring cells. Furthermore, the presence of schizocytes in the peripheral blood smear led to the diagnostic hypothesis of cancer-related microangiopathic haemolytic anaemia. The bone marrow biopsy highlighted the presence of gastric carcinoma signet ring cells in medullary stroma, accounting for the severity and persistence of blood cytopenias (figure 1). Despite treatment with plasmapheresis, since there were no clinical conditions to start chemotherapy, the patient died 42 days after diagnosis.
{kind=link}
(A) Area of signet ring cells invading the medullary stroma; (B) CK 7 colouration, a marker of proximal gastrointestinal epithelia, highlighting the process described in (A); (C) signet ring cell's embolus in medullary vascularisation; (D) CD34 colouration of vascular wall accentuating the process of signet ring cell's embolisation.
Myelophthisis is the term used for describing the medullary invasion by foreign elements (eg, infection, neoplasm), with functional impairment and ultimately leading to total bone marrow aplasia. Gastric carcinoma invading medullary tissue, particularly the signet ring cell type, is a rare event and is frequently associated with poor prognosis.1 It can be associated with severe microangiopathic haemolytic anaemia with a complex and multifactorial physiopathological mechanism that is not yet fully understood.1 ,2
The only effective treatment seems to be chemotherapy, although in some anecdotical cases, plasmapheresis has been used.1 ,2 However, despite treatment, survival does not usually exceed 2 months after the diagnosis has been made.1 ,2
Learning points
-
Despite its rarity, medullar invasion with refractory cytopenias can be the inaugural manifestation of gastric carcinoma with signet ring cells.
-
Bone marrow histopathology presents key features such as areas of carcinoma cells in the stroma and vascular embolisation.
-
Chemotherapy seems to be the only effective treatment, but prognosis in the majority of cases, despite treatment, is poor.
Acknowledgments
The authors thank Dr Lucília Monteiro for the indispensable contribution to this article.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Correction