Article Text

Statistics from Altmetric.com
Description
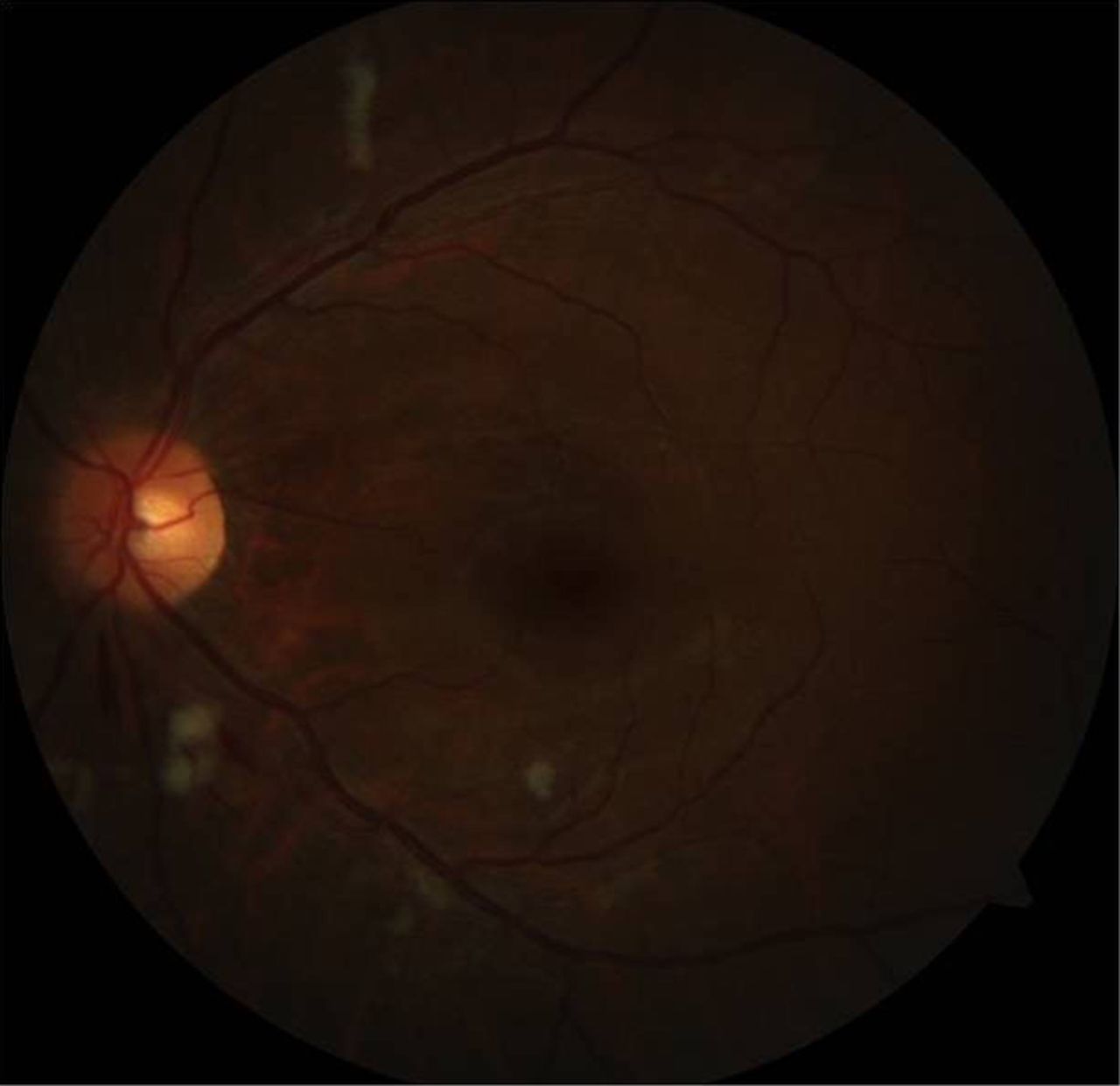
A 35-year-old Asian man presented with acute vision loss in the right eye. On examination, the best corrected visual acuities were 20/50 in the right eye and 20/25 in the left eye. Anterior segment examination was normal, intraocular pressures were 18 mm Hg in both eyes and there was no pupillary abnormality. Fundus examination of the right eye revealed an area of retinal papillomacular infarction with associated oedema due to cilioretinal artery occlusion illustrated on colour image and optical coherent tomography (figure 1). Fundus examination of the left eye showed multiple retinal haemorrhages with cotton wool spots (figure 2). Fluorescein angiography revealed delayed filling of the cilioretinal artery, consistent with cilioretinal artery occlusion (figure 3). Further examination revealed severe systemic hypertension (229/170 mm Hg) with a regular heart rate of 98 bpm. He was sent to the emergency room for lowering blood pressure and was admitted to cardiology to rule out secondary hypertension. Left ventricular hypertrophy was demonstrated on echocardiogram. No significant findings were identified by renal angiogram and brain CT. There was no evidence of secondary hypertension. After 8 weeks, retinal changes were completely resolved with improvement of vision in his right eye to 20/30.
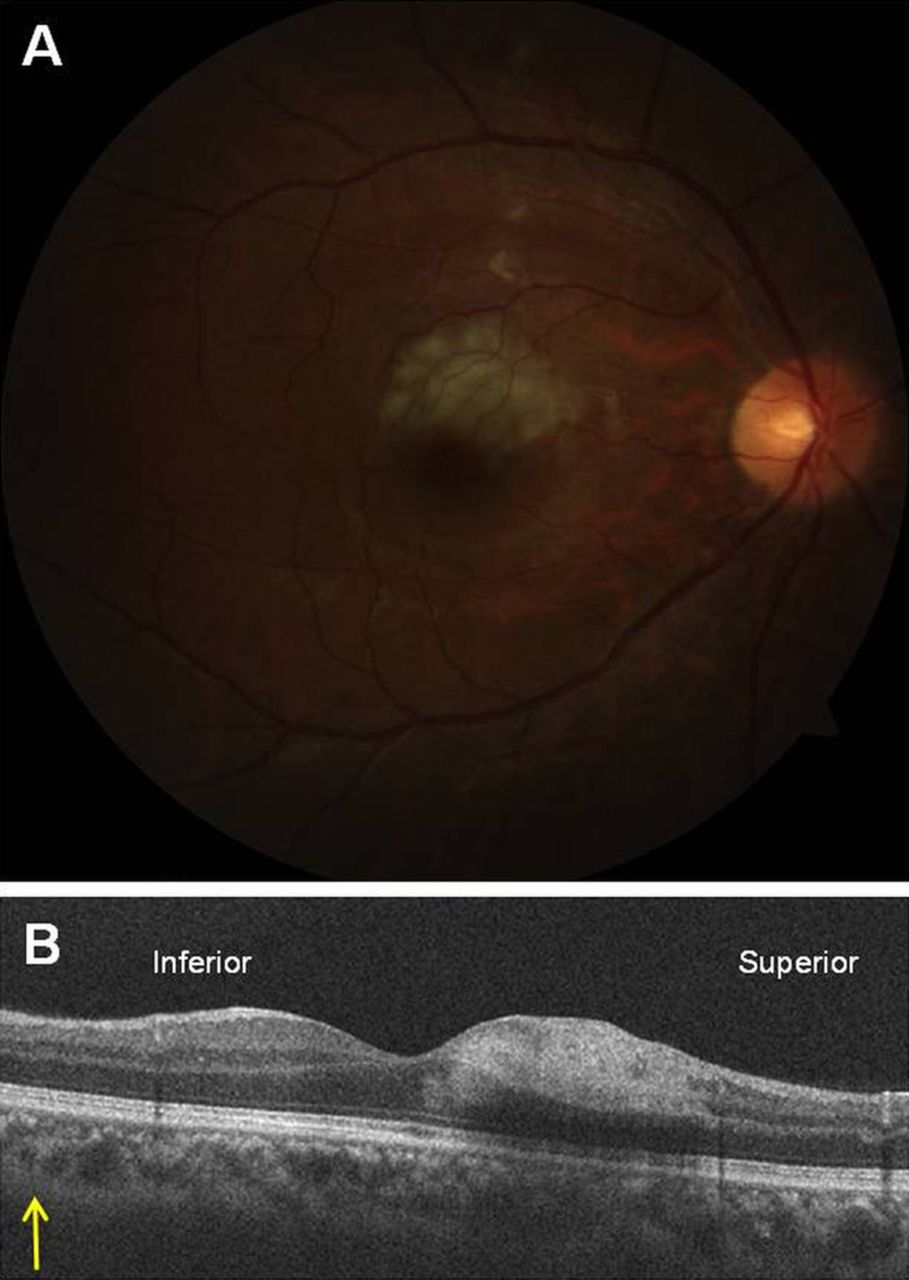
(A) Fundus photograph of the right eye showing superficial retinal whitening along the course of the cilioretinal artery. (B) Optical coherence tomography revealing a hyper-reflectivity of the inner retinal layers corresponding to a retinal infarction.

Fundus photograph of the left eye showing multiple retinal haemorrhages with cotton wool spots.

{kind=link}
{kind=link}
{kind=link}
Fluorescein angiography demonstrating poor filling of the obstructed cilioretinal artery and retinal capillary non-perfusion within the area of distribution of the vessel.
Cilioretinal artery occlusions occur in three clinical settings: as an isolated occlusion, in association with central retinal vein occlusions and in conjunction with anterior ischaemic optic neuropathy.1 Interestingly enough, in the above case hypertensive crisis and associated retinopathy were the only clinical findings manifested with no other signs of underlying vascular occlusive disease.
Learning points
-
Isolated occlusion of the cilioretinal artery is a rare entity as it typically presents in association with central retinal artery or vein occlusion.
-
Although diagnosis of isolated cilioretinal artery occlusion is made without difficulty, the underlying pathogenic mechanism remains difficult to explain due to the various phenomena revealed by the increased arterial pressure.
Footnotes
-
Contributors S-UP, S-JL and MK treated the patient and in doing so acquired the case data. They were also involved in the drafting of the manuscript. All the authors read and approved the final version of the manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.