Article Text

Statistics from Altmetric.com
Description
A full-term male baby was born to non-consanguineous parents. At birth his growth parameters were appropriate for age. On examination he had hypertelorism, broad nasal root and a cleft lip. Cranial ultrasound at birth was grossly normal except for partial agenesis of the corpus callosum. The cleft lip was repaired at 6 months of age. As part of the preoperative check, MRI of the brain was carried out. However it remained unreported. At 2 years of age (figure 1) he presented with recurrent nasal block and sleep disturbances. A detailed rhinoscopic examination showed a glistening mass in the right posterior nasal cavity and choana, causing a near total airway obstruction. Systemic examination was unremarkable. He had a normal ophthalmological evaluation. MRI carried out at 6 months was reviewed and showed a transsphenoidal encephalocele (TSE) with partial agenesis of the corpus callosum (figure 2). Neurosurgical opinion was sought and the consensus was to postpone surgery till second decade of life in view of the high-risk of hypothalamo-pituitary dysfunction following repair of the encephalocele.

Facial dysmorphism showing hypertelorism, broad nasal root and a cleft lip (repaired).

{kind=link}
{kind=link}
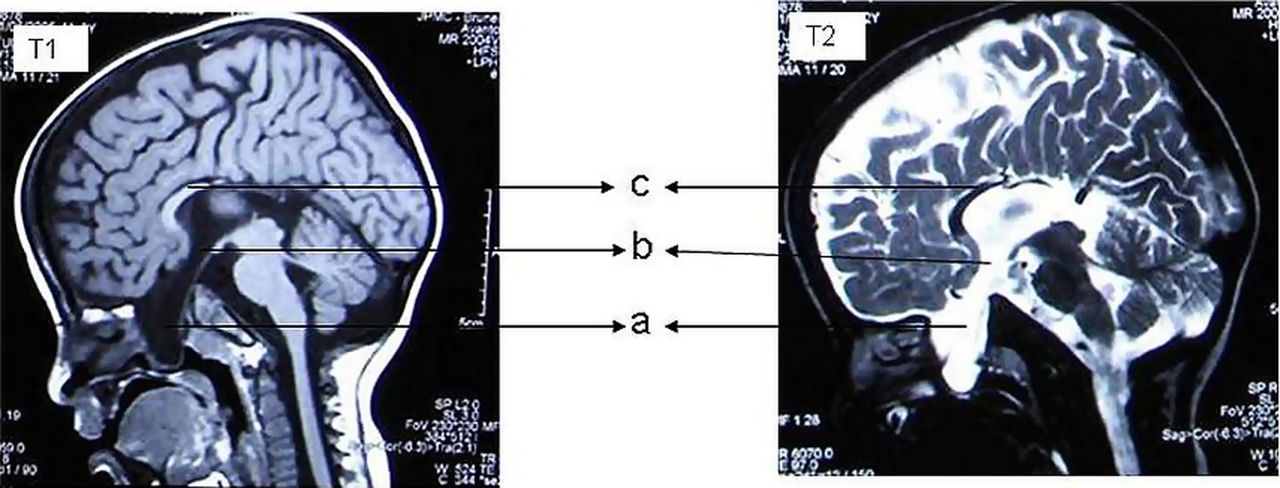
Sagittal T1-weighted and T2-weighted sequences showing the presence of a large cerebrospinal fluid-filled polypoidal lesion (A) extending through the anterior cranial fossa (B) and projecting into the nasopharynx. It is consistent with a transsphenoidal encephalocele. A normal pituitary gland is not visualised and partial agenesis of the corpus callosum (C) is noted.
Basal encephalocele (BE) occurs due to herniation of neural elements including pituitary gland or optic apparatus, through a defect in the skull base. TSE represents less than 5% of all BE with an estimated incidence of 1 in 700 000 live-births.1 Clinical presentation is most often insidious except in those cases where a large herniation protrudes through the epipharynx. They are often associated with hypertelorism, broad nasal root, cleft lip/palate, optic nerve anomalies and agenesis of the corpus callosum.2 Non-contrast CT scan of the head can delineate the bony defects. MRI with contrast enhancement is useful in identifying any neural or vascular elements in the herniated encephalocele.
Learning points
-
The presence of midline craniofacial anomalies in association with symptoms of nasal obstruction, persistent rhinorrhoea, visual deficits and/or endocrine dysfunction should alert physicians to the possible presence of basal encephalocele.
-
If conservative management is planned a notification to his school teacher to keep him away from contact sports and to physicians treating him to avoid nasal suctioning is recommended.
-
Indication for surgical intervention includes significant obstruction of respiratory pathway, repeated meningitis, rhinorrhoea and progressive visual defect attributable to the lesion. Endoscopic route is preferred because of the high rate of postoperative hypothalamo-pituitary dysfunction following transcranial approach.1 ,3
Acknowledgments
The authors would like to express their gratitude to Dato Dr N Ravindranathan, Senior Consultant OMF Surgeon, RIPAS Hospital, Brunei, Darussalam for referring this case to them.
Footnotes
-
Contributors All authors contributed to the preparation, editing and finalisation of the manuscript and figures.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.