Article Text

Summary
Acinic cell adenocarcinoma (ACC) is a low-grade malignant salivary neoplasm that constitutes approximately 17% of all primary salivary gland malignancies. In the head and neck region, the parotid gland is the predominant site of origin and ACC is usually more frequent in women than men. Previous radiation exposure and familial predisposition are some of the risk factors for ACC. ACCs rarely involve minor salivary glands constituting only 13–17% of all minor salivary gland tumours. Generally, a slowly enlarging mass lesion in the tail of the parotid gland is the most frequent presentation. ACC has a significant tendency to recur, metastasise and may have an aggressive evolution. Therefore, a long-term follow-up is mandatory after treatment. Here we report the case of a woman in her 60s with an ACC in association with the labial minor salivary gland, presenting in the post-treatment period of squamous cell carcinoma of the tongue.
Statistics from Altmetric.com
Background
Acinic cell adenocarcinoma (ACC) is a malignant salivary gland tumour recognised almost a century ago. It has been described as an adenocarcinoma predominantly of the parotid gland with malignant neoplastic epithelial cells resembling serous acinar and salivary ductal cells.1 The WHO classifies it as a malignant epithelial carcinoma with commonly low-grade behaviour.2
Salivary gland carcinomas account for 0.6% of all cancers with acinic cell carcinoma constituting about 1–6% of all salivary gland neoplasms.3 In adults, this tumour is the third most common epithelial malignancy of the salivary gland closely following mucoepidermoid carcinoma and adenoid cystic carcinoma.4
In the present case, the tumour was diagnosed in an elderly woman in the post-treatment period of squamous cell carcinoma (SCC) of the tongue which was diagnosed 10 years ago.
In the few case series on ACC of the minor salivary glands, its malignant behaviour is infrequently described. 4 ,5 Although it is established that this group of lesions are low-grade adenocarcinomas, they possess a significant tendency to recur, to produce local and distant metastases and may result in an aggressive course.
Reports show that acinic cell carcinomas can potentially undergo dedifferentiation. Dedifferentiation in acinic cell carcinomas has been found to occur in recurrent tumours secondary to radiation and more commonly in the solid and microcystic variants of this tumour. As in our case, the lesion had developed in the post-treatment period of SCC of the tongue which incidentally, was also of the solid variety of ACC having occurred in the labial minor salivary gland. Therefore, a long-term and regular follow-up is mandatory after treatment of such cases.
Case presentation
A female patient in her 60s reported to the clinic with a right labial mass of 5 years duration that was otherwise completely asymptomatic and of a stable size (figure 1). The patient had a history of SCC of the right side of the tongue for which a partial glossectomy was performed (figure 2) accompanied by head and neck radiotherapy 10 years ago. She had received a dose of 60–65 Gy for a duration of 6 weeks. Her medical history was otherwise unremarkable.

A diffuse swelling is seen on the right side of the upper lip, about 1 cm below the ala of the nose.

Photograph shows tongue postpartial glossectomy of the right side as part of treatment for squamous cell carcinoma.
On extraoral examination, a diffuse swelling was seen on the right lip extending 0.5 cm from the ala of the nose to the vermillion border of the lip superoinferiorly and 1 cm from the midline to 1 cm from the angle of the mouth mesiodistally measuring 2×2 cm in diameter. The skin over the swelling was normal. On palpation, the swelling was soft to firm in consistency.
Intraoral examination revealed a well demarcated nodular mass on the right labial mucosa measuring 4×2 cm in diameter. On palpation it was soft to firm in consistency. Small varices were seen traversing the swelling (figure 3).

A well-demarcated swelling seen on the right labial mucosa, which is nodular with a normal appearing oral mucosal surface.
The nodule on the labial mucosa with a non-ulcerated mucosal surface was provisionally diagnosed as an adenoma. The lesion was surgically excised.
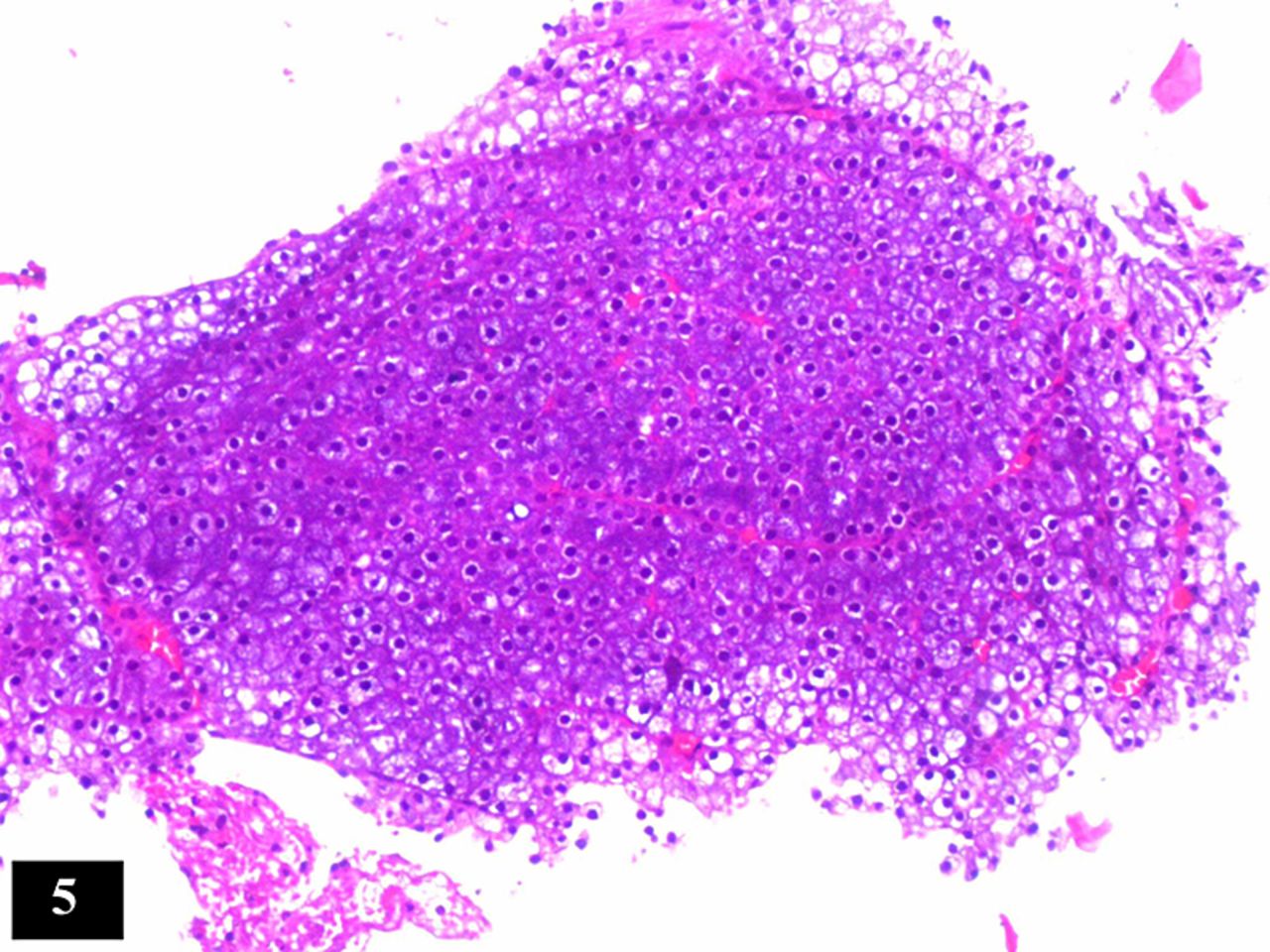
Macroscopic examination revealed a non-encapsulated lobular mass approximately 2.5 cm in diameter with irregular friable areas which appeared haemorrhagic. Microscopic examination on a scanner view revealed solid areas of tumour cells which were arranged in large sheets and lobules (figure 4). The cells were secretory epithelial cells bearing resemblance to serous acinar or secretory cells. These cells presented with a classical round hyperchromatic nucleus in each cell. Their nuclei have been referred to as ‘blue dots’ of the tumour by some authors (figure 5).

Photomicrograph showing a lobule of tumour cells arranged in organoid pattern (H&E ×10).

Photomicrograph showing classic blue dot tumour with round to polygonal neoplastic cells containing a hyperchromatic round blue nucleus (H&E ×10).
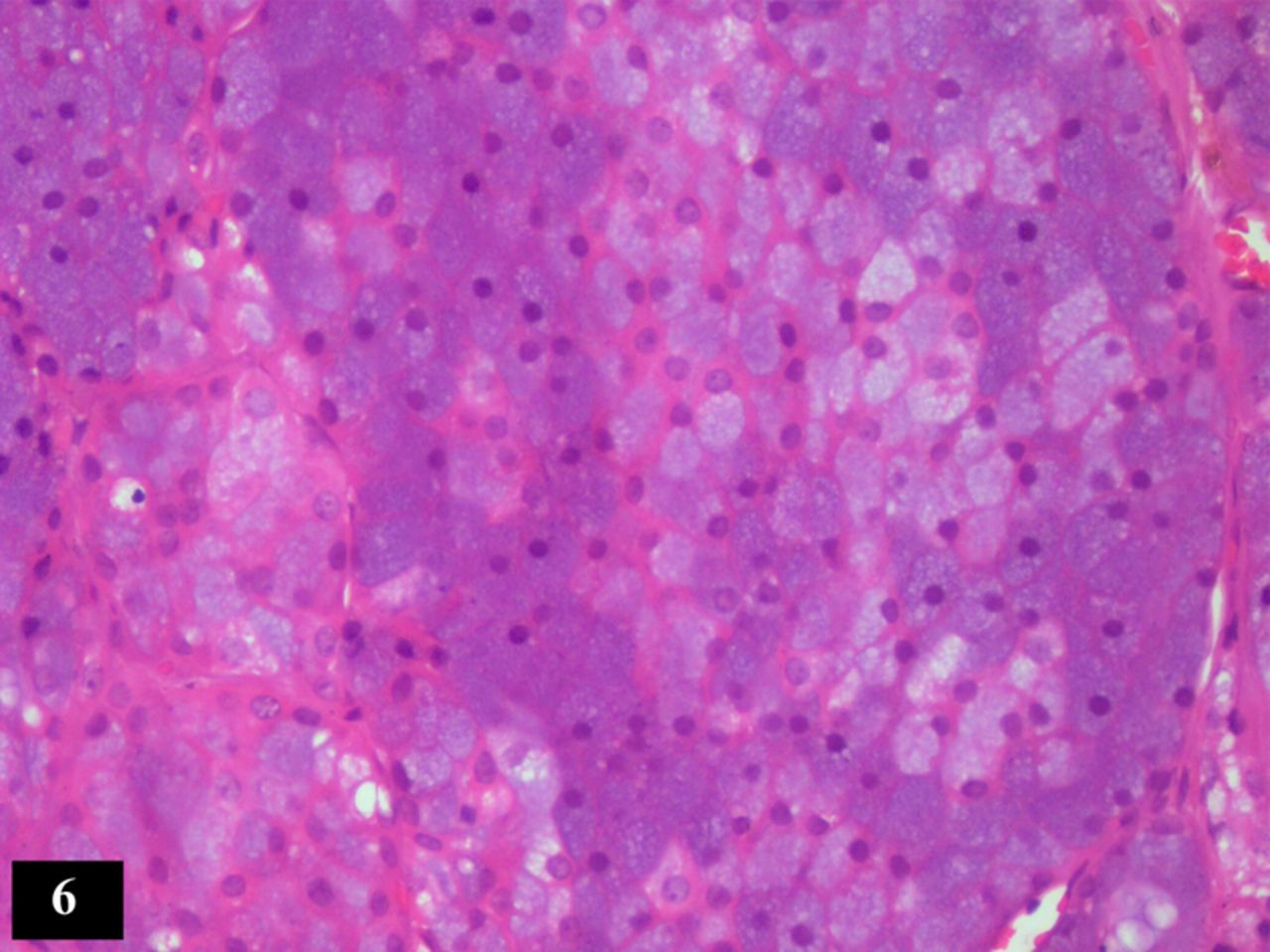
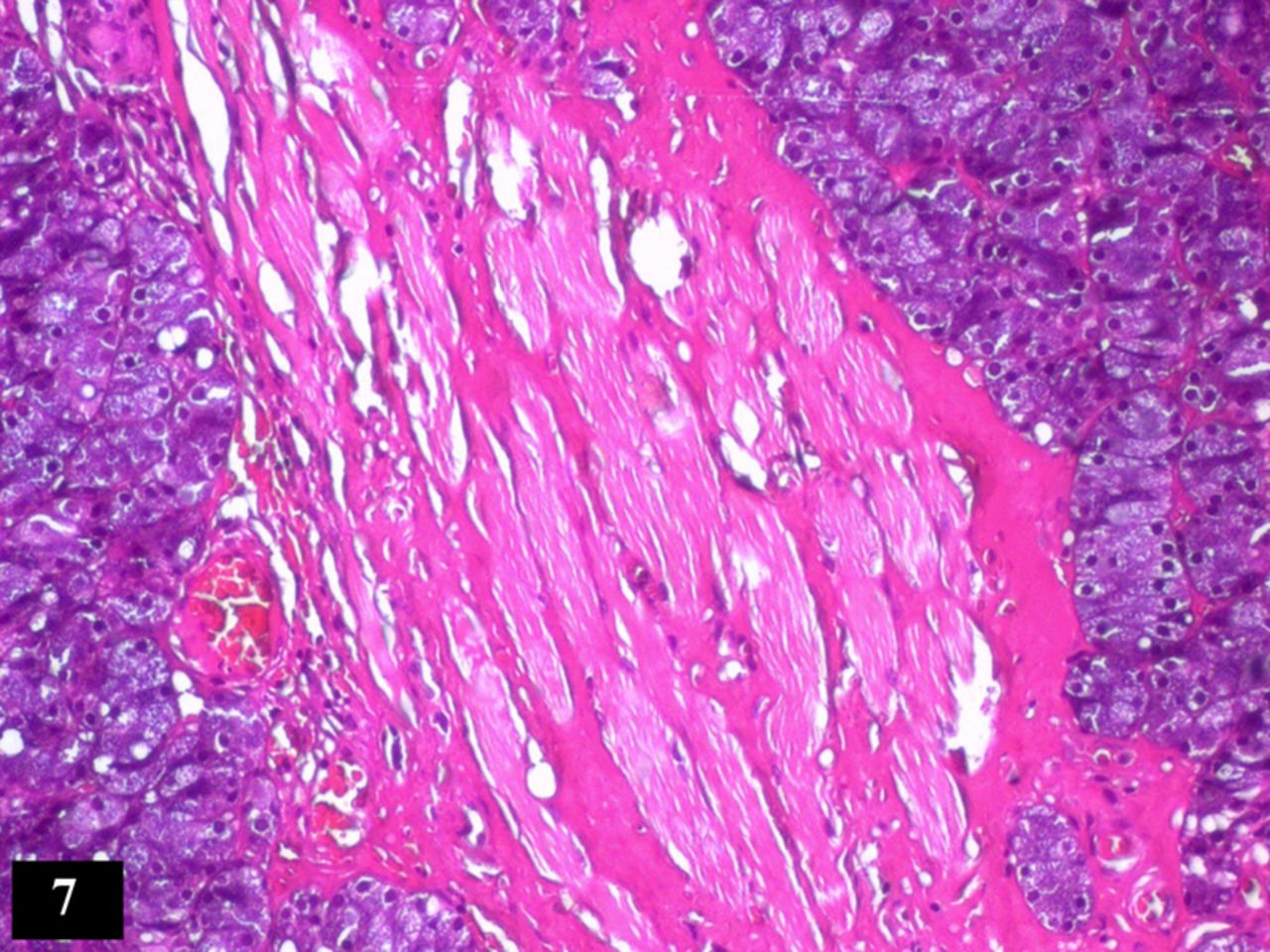
The neoplastic cells were arranged in an ill-defined organoid pattern separated by numerous delicate connective tissue septae and newly formed capillaries. A closer examination on a higher power revealed a second population of cells which appeared paler and polygonal with a large vesicular nucleus (figure 6). In one area the cells were seen invading in between the skeletal muscle fibres (figure 7).

Photomicrograph reveals two populations of tumour cells showing both dark staining oval cells and slightly larger pale staining polygonal cells (H&E ×20).

Lesional tissue cells show skeletal muscle invasion and degenerating skeletal muscle fibres (H&E ×10).
Staining with periodic acid-Schiff (PAS) special stain, clearly showed two types of cells: one, a set of darkly stained cells with a prominent round hyperchromatic nuclei and granular cytoplasm, the other, where cells were paler and polygonal with vesicular nuclei (figure 8).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
PAS staining shows positively stained cytoplasm of tumour cells with hyperchromatic round nucleus (PAS ×20).
This classical histopathological picture aided in diagnosing the case as a ‘solid variant’ of ACC.
Differential diagnosis
Generally for the microcystic and papillary microcystic variants of ACC, a differential diagnosis of the recently described entity; mammary analogue secretory carcinoma (MASC) is considered. Our case was a solid variant with large and small sheets of tumour cells. No ductal, follicular or cystic pattern was evident.
MASCs show localisation of PAS stain with very minimal intracellular staining. In our case, the PAS positivity was strongly observed in the cellular component which was rich in zymogen granules (refer figure 8).
Treatment
The patient was surgically treated for the tumour. The lesion was excised en masse under general anaesthesia with a 1 cm margin of normal tissue. Profuse bleeding was encountered on surgical exploration. Postoperative radiotherapy was advised. The patient had received a dose of 55–60 Gy for 5 weeks duration.
Outcome and follow-up
The patient has shown no signs of recurrence or any other symptoms until after 2.5 years of follow-up at regular intervals of 3 months.
Discussion
ACC is a low-grade salivary gland tumour which shows proliferation of acinar cells of serous type arranged in various patterns. It accounts for 6–10% of all salivary gland tumours.5
ACC obtained recognition as a malignant tumour in 1953 with the report of Buxton, Foote and Frazell, though the first description of the tumour dates back to 1892 by Wane D.3 ,6
ACC is rare and uncommon in the minor salivary glands (9–13%), more commonly occurring as a tumour involving parotid (83–86.3%),1 ,5 ,7 predominantly seen in women (58.8%) at an average age of 44 years.1
Our case presented as a labial mass involving the minor salivary gland in a female patient in her 60s. Gender, location and age were in agreement with most of the literature.1 ,4 ,7
Numerous possibilities have been enlisted as aetiological factors for this low-grade malignancy. Familial predisposition, endogenous female hormones and previous radiation exposure are some common factors considered. Genetic alteration of chromosomes 4p, 5q, 6p and 17p are said to be associated with tumour-suppressor genes and oncogenesis have been found to be linked with ACC. Reports of oestrogen and androgenic receptors in cases of ACC also deserve mention, justifying female predominance. Previous radiation exposure for treatment of various carcinomas has also been cited as a cause for ACC.7
In the present case, therapeutic radiation was received by the patient as a part of treatment for SCC tongue along with surgical approach. The current tumour had arisen in the line of radiation, questioning the possibility of acinic cell carcinoma developing due to radiotherapy. Our patient was treated for SCC 10 years ago and the tumour had developed in the postradiation period as the patient was aware of a slow growing tumour since approximately 5 years.
There are many reports of salivary gland tumours as second neoplasms8 and radiotherapy for oral cancer as a risk for such second primary malignancies.9 ,10 Occurrence of salivary gland tumours due to previous radiotherapy to the head and neck suggests that there is a strong association between exposure to radiation and tumour development in various cases.11 ,12
In this particular case, as the patient had developed the tumour in the line of radiation in the postsurgical period, the possibility of the tumour associated with radiation cannot be ruled out.
Histologically ACC may present in various morphological growth patterns such as solid, microcystic, papillary cystic and follicular. The solid pattern of acinic cell carcinoma is referred to as ‘classical pattern’ though the microcystic pattern is more commonly seen. The papillary cystic and follicular variant being less common than the solid pattern.1 ,13 The present case showed a classical solid pattern with cells arranged in large sheets in organoid pattern separated by thin fibrovascular connective tissue septa.
The cell types seen in acinic cell carcinoma are acinar/serous acinar, intercalated duct like, vacuolated, clear and non-specific glandular types. A variation of morphological pattern and cell type can be seen in any specific tumour.1 Our case showed a good population of serous acinar cells. A closer examination revealed a second population of cells which appeared paler and intercalated duct like along with a few non-specific glandular, vacuolated clear cells. A diagnosis based on these findings resulted in categorising the tumour as a well differentiated acinic cell carcinoma-solid variant. ACCs are referred to as ‘blue dot tumors’ because of acinar cells displaying a large round basophilic nucleus in a granular cytoplasm.13 This feature was very well appreciated in the present case.
The tumour cells generally express their aggressive behaviour by demonstration of invasion in the tissue and presence of pleomorphism, mitosis, necrosis of the cells. Neural invasion and tissue hyalinisation has also been reported in some cases. We observed infiltration of the skeletal muscle bands by the tumour cells, leading to degeneration of the muscle fibres at a few foci.
ACCs have been divided into three grades:
-
Group 1: Low grade—completely encapsulated tumour without local infiltration.
-
Group 2: Moderate grade—tumour shows signs of capsular invasion.
-
Group 3: High grade—infiltration of the surrounding tissues and presence of papillary cystic areas.14 ,15
ACC shows strong positivity to PAS staining in the acinic cell component because of zymogen granules. This finding in our case was clearly observed in the acinar cells whereas the other cell population remained palely stained in agreement with other reports.16
The papillary cystic, microcystic and follicular variants require consideration of differential diagnosis which includes a host of salivary gland tumours.3 ,17 Owing to a solid variant, like in our case is more easily recognised for histopathological diagnosis.
These tumours are treated with surgery with an intraoral or extraoral approach depending on the extent and location.17 Andreoli et al6 clearly assert the compromised and limited role of radiation in the treatment of ACC. According to many authors, ACCs are not radiosensitive and therefore radiotherapy is generally recommended only for tumours with large size, local tissue invasion and multiple lymph node positivity.17
ACCs are indolent low-grade tumours but can be quite persistent leading to local recurrence and metastasis. These phenomena can be noted commonly after 3–10 years and may resurface after 20–30 years.5 Our patient was treated with surgical excision with a wide margin and has had a disease free survival after 2.5 years of treatment. We recommend a long-term follow-up for all cases of ACC irrespective of their histological variants and site.
Conclusion
We report a case of solid ACC arising in a minor salivary gland, which is comparatively a rare location; as the parotid gland accounts for 85% of this tumour. The case also shows a possible link between radiation (postsurgical treatment of the SCC of the tongue) and the occurrence of this salivary gland neoplasm; hence validating radiation as a possible aetiology for ACC.
Learning points
-
Acinic cell adenocarcinoma, though known to be a low-grade tumour, can be invasive and is therefore currently considered as an aggressive lesion.
-
The probability of an acinic cell carcinoma having occurred secondary to radiation therapy for squamous cell carcinoma of the tongue cannot be ruled out.
-
Acinic cell carcinomas are vascular tumours and this could explain the profuse bleeding encountered during surgery.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.