Article Text

Statistics from Altmetric.com
Description
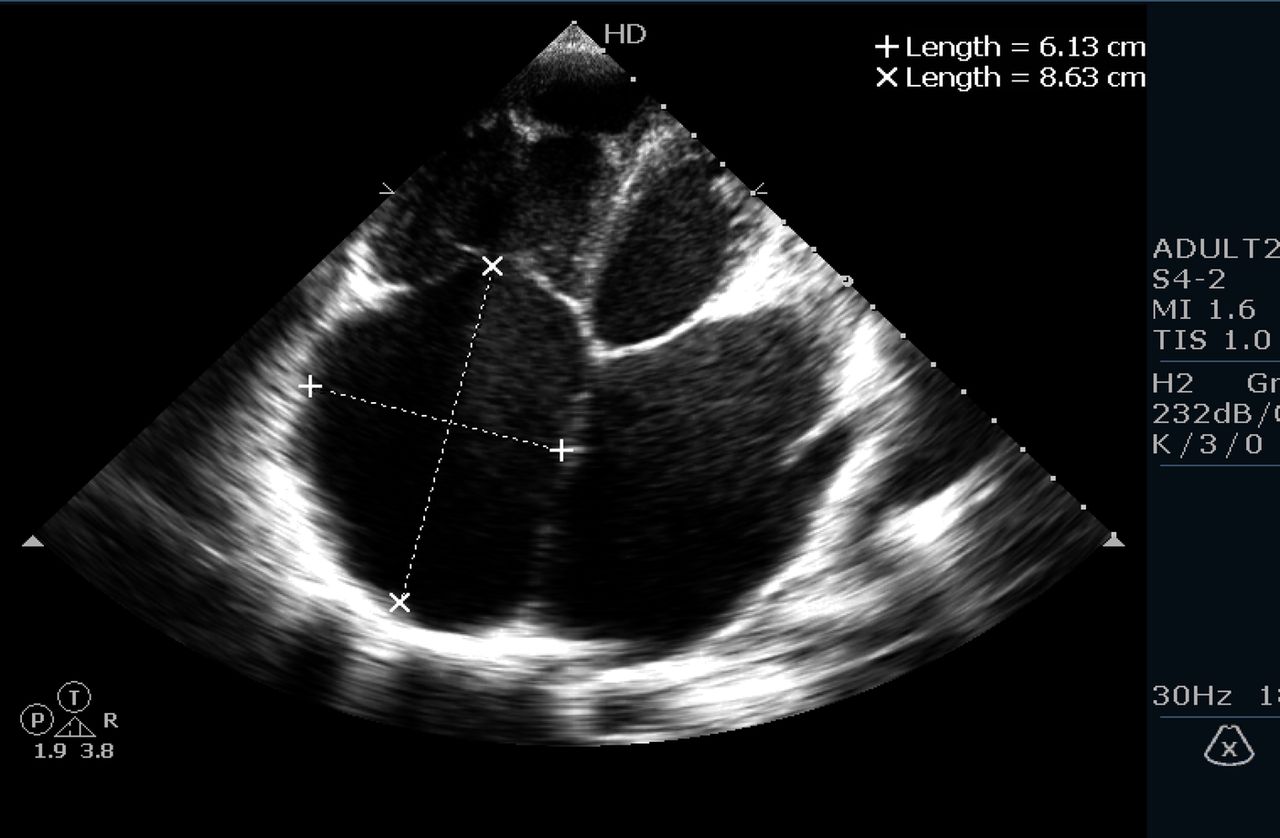
A 19-year-old man presented with New York Heart Association class II heart failure with a history of rheumatic fever in childhood. He was on regular penicillin prophylaxis, diuretics, vasodilators and β blockers. On examination there was grade IV/VI pansystolic murmur at the apex radiating to the axilla, grade III/VI pansystolic murmur at left sternal border fourth intercostal space (increasing on inspiration). Mean jugular venous pressure was elevated (prominent v waves) with gross pedal oedema. A 12-lead ECG revealed atrial fibrillation with a controlled ventricular rate. A transthoracic echocardiogram revealed severe mitral stenosis (videos 1 and 2), moderate mitral regurgitation (video 3), severe torrential tricuspid regurgitation (video 4) and mild aortic regurgitation (video 5).There was severe right ventricular dysfunction with adequate left ventricular function. Mitral valve leaflets were thickened and fused with commissural fusion and mild subvalvular disease (figure 1). The mitral valve orifice area was 0.5 cm2 (figure 1) with gradient of 29/24 mm Hg (figure 2). The left atrium was giant with a size of 7.12×8.66 cm (figure 3). The right atrium was also giant with a size of 6.13×8.63 cm (figure 4). Pulmonary pressure was 115 mm Hg (figure 5). The right and left atrial area were 35 and 42 cm2 (normal range <20 cm2), respectively. The calculated right and left atrial volumes were 198 and 165 mL (normal range 22–52 mL), respectively. The patient underwent mitral valve replacement, tricuspid valve annuloplasty and left atrial reduction and doing well currently.

Basal parasternal short axis view showing mitral valve area.
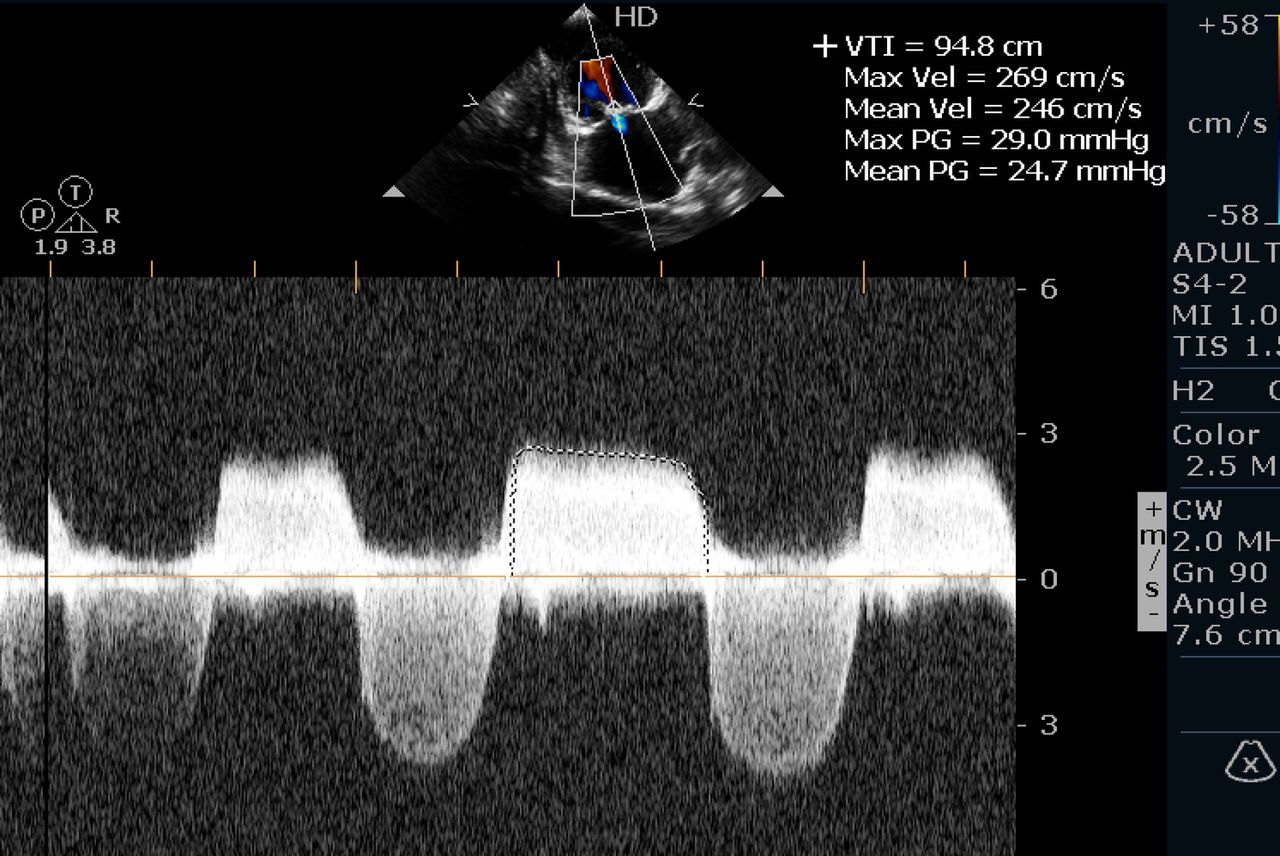
Apical four-chamber view with continuous wave Doppler across mitral valve with gradient.

Apical four-chamber view showing left atrial dimensions.

Apical four-chamber view showing right atrial dimensions.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Apical four-chamber view with continuous wave Doppler across tricuspid valve with gradient.
Parasternal long axis view showing typical hockey stick mitral valve.
Apical 4 chamber view showing severe mitral stenosis with valvar fusion,noncoapting tricuspid valve leaflets and dilated left and right atrium.
Apical 4 chamber view with colour doppler across mitral valve showing turbulent forward flow across mitral valve with moderate mitral regurgitation.
Apical 4 chamber view with colour doppler across tricuspid valve showing severe tricuspid regurgitation with right ventricular dysfunction.
Apical 5 chamber view with colour doppler showing mild aortic regurgitation.
This case is a typical example of rheumatic heart disease found in young population in countries like India. Outstanding feature is giant left and right atria both in same patient.
A giant left atrium1 ,2 can be found in 19% of patients requiring surgery for mitral valve. Any left atrial diameter more than 6.5 cm is giant. A giant left atrium (LA) increases the risk of surgery on mitral valve. It is observed that pulmonary oedema occurs less commonly in patients with multiple sclerosis (MS) who have giant LA. Mitral regurgitation is more commonly associated with giant LA than MS.
A giant right atrium3 ,4 can be due to Ebstein anomaly, pulmonary hypertension or tricuspid regurgitation. In our case severe tricuspid regurgitation with pulmonary hypertension was the cause of the giant RA.
Learning points
-
Rheumatic heart disease is the typical cause of a giant left atrium especially in patients having mitral regurgitation.
-
Patients of rheumatic heart disease with a giant left atrium are protected from pulmonary oedema to some extent.
-
Rheumatic heart disease with a giant right atrium can be seen in patients with severe pulmonary hypertension.
Acknowledgments
The authors would like to thank their institute.
Footnotes
-
Contributors HM and RC diagnosed the case and was involved in the article preparation. SB was involved in corrections. CNM gave guidance and was involved in the final approval of the article.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.