Article Text

Statistics from Altmetric.com
Description
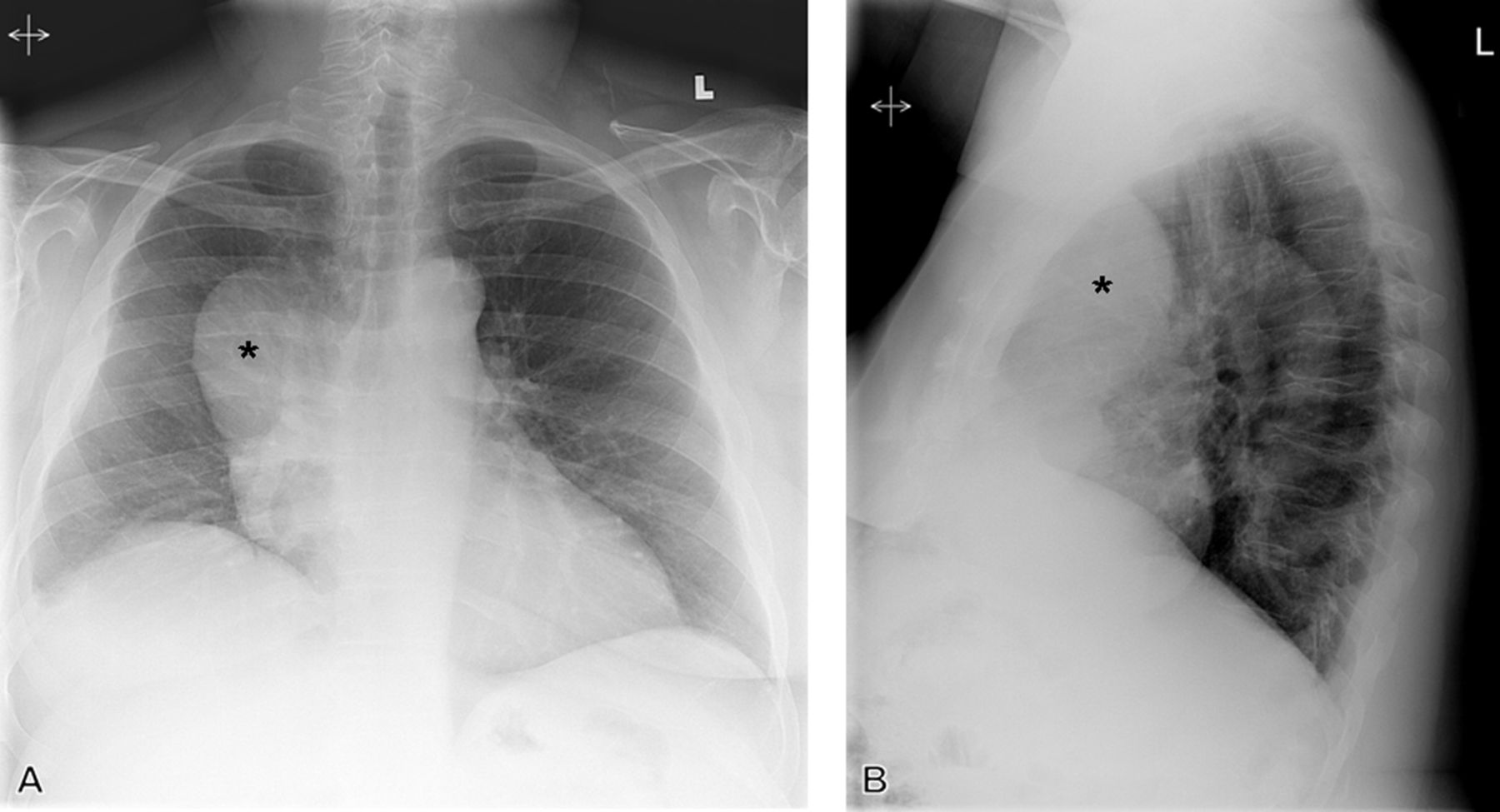
An asymptomatic middle-aged man presented for routine preoperative chest radiographs prior to the resection of a Masson's tumour of the frontal sinus. The chest radiographs revealed a large anterior mediastinal mass (figure 1). A CT scan of the chest was subsequently performed for further evaluation, demonstrating a cystic mass abutting the right anterior mediastinum with homogenous fluid attenuation (figure 2). A catheter could be seen extending from the soft tissues of the neck and coiling within the mass. Correlation with the head CT led to a diagnosis of pleural cerebrospinal fluid (CSF) pseudocyst associated with a ventriculopleural shunt. On further discussion with the patient, it was revealed that he had undergone ventriculopleural shunt placement for hydrocephalus at an outside institution following an episode of traumatic subarachnoid haemorrhage 20 years earlier. No further intervention was required, as the patient remained asymptomatic.

Posteroanterior (A) and lateral (B) radiographs of the chest demonstrate a rounded anterior mediastinal mass (asterisk). Differential considerations at the time of interpretation included lymphoma, thymoma or germ cell tumour.

{kind=link}
{kind=link}
Contrast-enhanced CT of the chest demonstrating a ventriculopleural shunt catheter extending into a pleural cerebrospinal fluid (CSF) pseudocyst. (A) Axial images demonstrate a loculated pleural fluid collection (asterisk) measuring 0 hounsfield units, representing simple fluid density. (B) Coronal reconstructions showing a catheter (arrow) extending from the right neck into the pleural fluid collection. (C and D) Sagittal and three dimensional reconstructions with right anterior ribs digitally subtracted showing the catheter (arrowheads) coiling within the pleural fluid collection. A CT scan of the head (not shown) revealed a ventricular shunt in the right lateral ventricle with catheter tubing extending down the right side of the head. This constellation of findings led to the diagnosis of a pleural CSF pseudocyst as a complication of a ventriculopleural shunt.
A CSF pseudocyst is a well-recognised complication of CSF diversion catheters that is most commonly associated with ventriculoperitoneal shunts.1 The ventriculopleural shunt is an alternative method of CSF diversion used when ventriculoperitoneal or ventriculoatrial shunts are not suitable due to adhesions, a history of peritonitis, ascites, peritoneal dialysis or failure of a prior ventriculoperitoneal shunt.2 Although uncommon, the ventriculopleural shunt is associated with a number of complications in the chest, including pleural effusion, empyema, tension hydrothorax, pneumothorax and rarely, as in this case, a CSF pseudocyst.2 An understanding of this alternative method of CSF diversion and awareness of the potential complications is essential when radiographic abnormalities of the chest are encountered in a patient with a ventriculopleural shunt.
Learning points
-
The ventriculopleural shunt is an alternative method of cerebrospinal fluid (CSF) diversion used when ventriculoperitoneal or ventriculoatrial shunts are not suitable due to adhesions, a history of peritonitis, ascites, peritoneal dialysis or failure of a prior ventriculoperitoneal shunt.
-
Complications of ventriculopleural shunting include pleural effusion, empyema, tension hydrothorax, pneumothorax and rarely a CSF pseudocyst.
-
Knowledge of these potential complications is essential when encountering an abnormality of the pleural space in a patient with a ventriculopleural shunt.
Footnotes
-
Contributors PCT was involved in conception and design, interpretation of imaging, and drafting the article and gave final approval of the version to be published. CS, WJR and TJM (senior author) were involved in analysis of the imaging, revising the article critically for important intellectual content, and gave final approval of the version to be published.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.