Article Text

Statistics from Altmetric.com
Description
A 57-year-old man was hospitalised in the emergency ward because of sudden appearance of nausea, vomiting, dizziness, nystagmus, motor aphasia associated to pain and cyanosis in the left arm. Doppler sonography detected a left omeral artery occlusion, due to acute embolism. The first brain CT scan was negative, but 24 h later evidenced multiple ischaemic infarctions in the brain (right cerebellar hemisphere, Broca's area; figure 1).
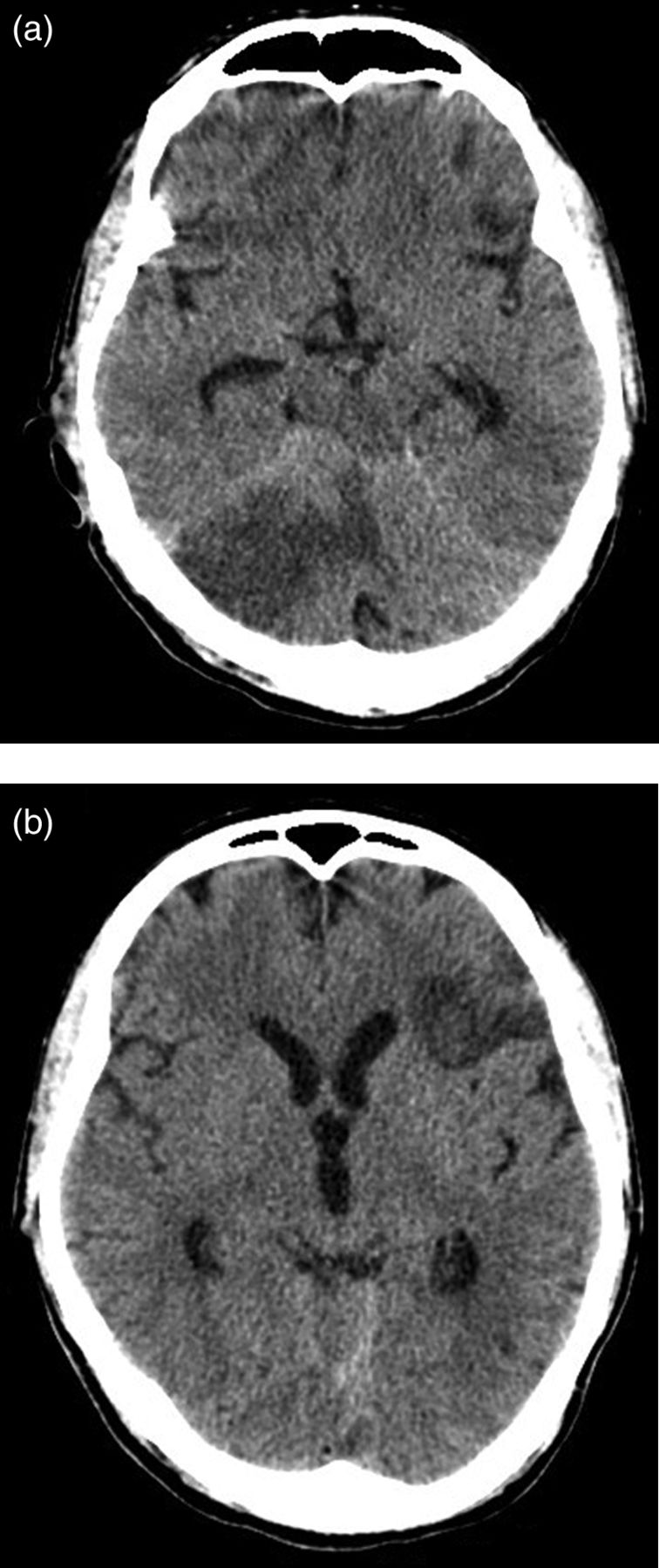
Embolic stroke. Brain CT scan after 24 h from admittance showing multiple ischemic areas in the cerebellum (vermis and right hemisphere; A) and in the pars opercularis of the inferior frontal gyrus (B).
Disseminated arterial multiple embolisms (involving in this case the brain and an upper limb) usually originate from fragments of cardiac or aortic thrombus. The CT angiography in the acute phase detected a floating thrombus in the ascending aortic arch and no concomitant lesions in the aortic wall or in the cerebral arterial vessels. There was no sign of isolated central nervous system vasculitis. The only cardiovascular factor detectable was hyperhomocysteinaemia; the entire autoimmunity panel (and especially antiphospholid antibodies) was negative.
Looking for causes of isolated ascending aortitis1,2 (related to congenital collagenopathies, to infectious or autoimmune diseases), we diagnosed a latent tertiary syphilis3. At admittance serological tests (RPR 1:25, TPPA 1:10240, IgM anti-Treponema Pallidum negative, total antibodies against Treponema pallidum >70.00), the absence of history and the absence of previous treatment with penicillin led to the diagnosis of latent syphilis. Concomitant viral infections (HIV, HBV and HCV) were excluded with adequate serological test. Lumbar puncture was not performed because of the urgent need for anticoaugulation. Despite the lack of histological confirmation (the patient did not undergo cardiothoracic surgery because of the favourable outcome) we concluded that the explanation was luetic aortic damage,4 which could have promoted the thrombus growth with consequent multiple symptomatic embolisms.
The patient was anticoagulated with continuous heparin infusion for several days followed by oral sodic warfarin (international normalised ratio (INR) 2.5–3) and treated with intravenous penicillin at the dose of 1 g every 6 h for 10 days. After 25 days, the floating thrombus completely disappeared (figure 2) and most of the neurological symptoms dramatically improved. After an 8-month follow-up, the patient's condition was stable and serological luetic antibodies decreased in accordance with the treatment (immunological scar).

{kind=link}
{kind=link}
Floating thrombus. CT angiography at admittance: axial CT scan (A) and coronal reconstruction (B) showing an ulcerated plaque in the aortic arch, complicated by acute massive thrombosis (18×11 mm). At control (C): after 25 days of anticoagulation the thrombus totally disappeared.
Learning points
-
Syphilis in developed countries is a re-emerging disease that can mimic many medical conditions and can be the underlying cause of serious cardiovascular disorders.
-
A floating thrombus in the aortic arch is an emergency that should be operated or anticoagulated immediately because of the high risk of sudden multiple embolisms.
Acknowledgments
The authors would like to thank Dr Lorenzo Coppo for his help in the clinical management of the patient and in the diagnostic procedure.
Footnotes
-
Contributors PR contributed in the conception and design, acquisition of data, analysis and interpretation of data; drafting the article; final approval of the version published. DM was responsible for the acquisition of the data, analysis and interpretation of the data; final approval of the version published. PF was responsible for the analysis and interpretation of data; drafting the article; final approval of the version published. RC was responsible for the revision of the paper for important intellectual content; final approval of the version published.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.