Article Text

Statistics from Altmetric.com
Description
Periostitis of long bones is a possible yet rare manifestation of vasculitides such as polyarteritis nodosa (PAN).1 We report on a periostitis revealing a PAN, an exceptional situation.2
A man in his 40s, with no medical record, presented with a 3-month history of bilateral leg pain, diffuse myalgias, weight loss and fatigue. Physical examination showed permanent pain in both thighs, with no signs of arthritis or muscle weakness. Erythrocyte sedimentation rate and C reactive protein (CRP) levels were elevated (96 mm and 304 mg/L, respectively). Immunological tests were found to be normal (antineutrophil cytoplasmic antibodies, antinuclear autoantibodies, complement, IgG, IgA and IgM levels).
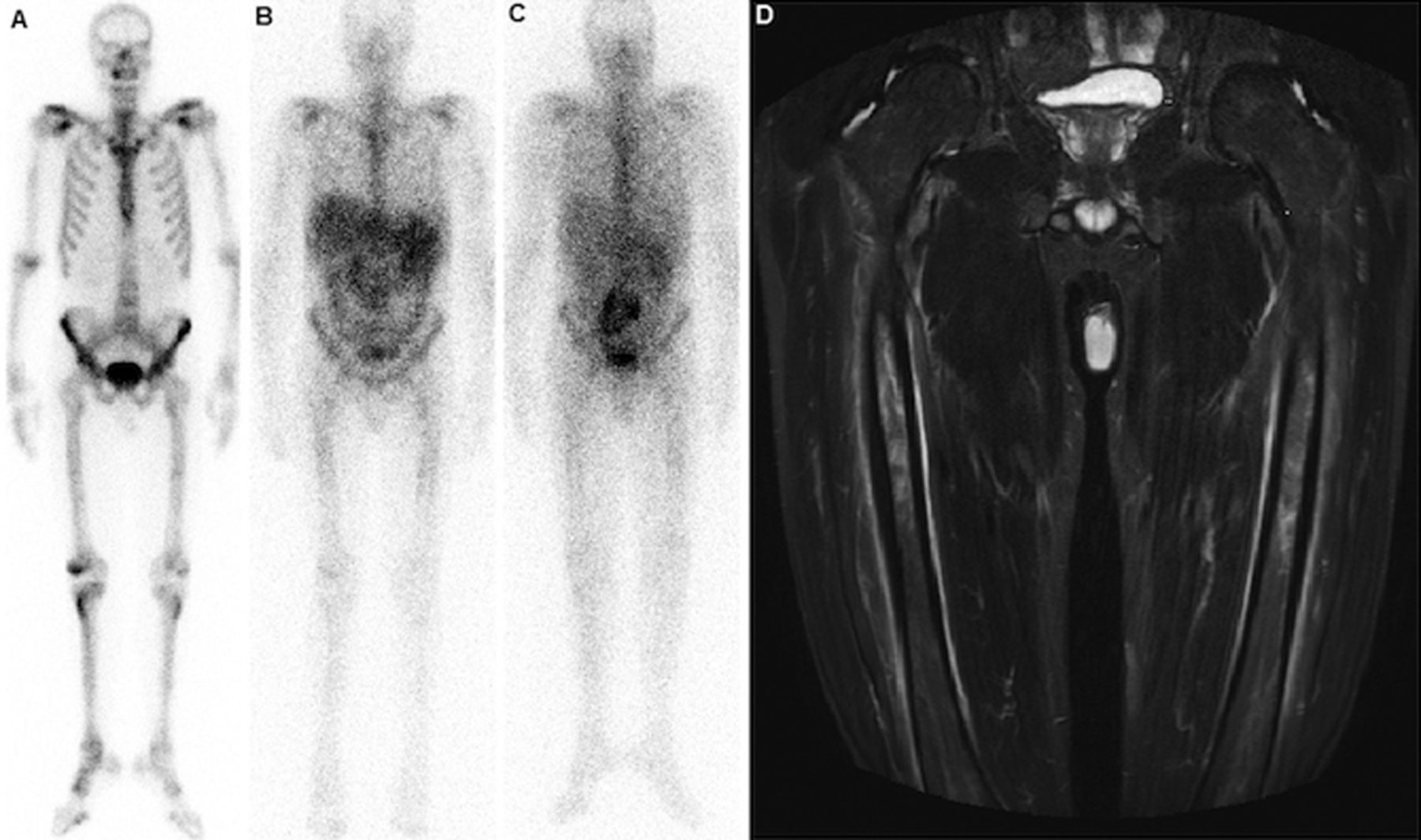
Femoral X-rays were normal. Bone scintigraphy (figure 1A–C), a useful first-line examination in detecting extra-articular involvement of inflammatory processes,3 showed uptake heterogeneities of both tracers on femoral diaphyses, due to inflammatory periosteal lesions, on whole-body scans obtained 6 (figure 1A and B) and 72 h (figure 1C) after injection of 580 MBq of 99mTc-HMDP and 110 MBq of 67Gallium. MRI of the lower limbs (figure 1D: short tau inversion recovery sequence, coronal section) showed circumferential hypersignals of femoral diaphyses, indicating active periosteal appositions. Quadricipital muscle biopsy showed no significant abnormality. An abdominal CT scan showed a left renal infarction and the coeliomesenteric arteriography, a left renal microaneurysm, confirming the diagnosis of PAN according to the 1990 American College of Rheumatology (ACR) criteria. Other explorations found no argument for another cause of periostitis (infection, neoplasm and other systemic diseases).

{kind=link}
Scintigraphic and MRI aspects of femoral periostitis in polyarteritis nodosa (A–C). Whole-body scans obtained 6 (A and B) and 72 h (C) after injection of 580 MBq of 99mTc-HMDP and 110 MBq of 67Gallium: mild uptake heterogeneities of both tracers on femoral diaphyses, due to inflammatory periosteal lesions. (D) MRI of the inferior limbs, short tau inversion recovery sequence, coronal section: circumferential hypersignal of both femoral diaphyses, indicating active-type periosteal appositions.
Oral corticosteroids (prednisone 1 mg/kg/day) led to a dramatic improvement of leg pain and weight loss. Twelve weeks later, the patient was asymptomatic and CRP was normal.
Learning points
-
Systemic vasculitides, such as polyarteritis nodosa, must be included in the differential diagnoses of periostitis of long bones.
-
Periostitis of long bones can be the revealing manifestation of PAN and the only sign of a relapse.
-
Bone scintigraphy is a useful first-line examination in detecting extra-articular involvement of inflammatory processes.
Footnotes
-
Contributors The final version of the manuscript has been seen and approved by all the authors and they have given necessary attention to ensure the integrity of the work.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.