Article Text

Statistics from Altmetric.com
Description
A 46-year-old woman presented to us with symptoms of breathlessness New York Heart Association class II for 6 months on and off with a history of rheumatic fever in childhood. She was diagnosed in the periphery as having rheumatic heart disease for 20 years. The patient was on regular injectable penicillin prophylaxis (injection penicillin 1.2 million units every 21st day), β-blockers with intermittent diuretics. Cardiac examination revealed low pitched mid-diastolic rumble grade III/VI at apex with normal S1.
Twelve-lead ECG showed atrial fibrillation with controlled ventricular rate. Echocardiogram revealed moderate mitral stenosis with severe subvalvular disease. Severe subvalvular fusion created double orifice appearance (figures 1 and 2). The combined mitral valve area of two orifices was approximately 1.5 cm2 (figure 3), gradient was only 8/5 mm Hg (figure 4). This valve was unsuitable for percutaneous valvotomy due to severe subvalvular disease (videos 1–4). The patient underwent mitral valve replacement with mechanical bileaflet valve. She is doing well on follow-up.
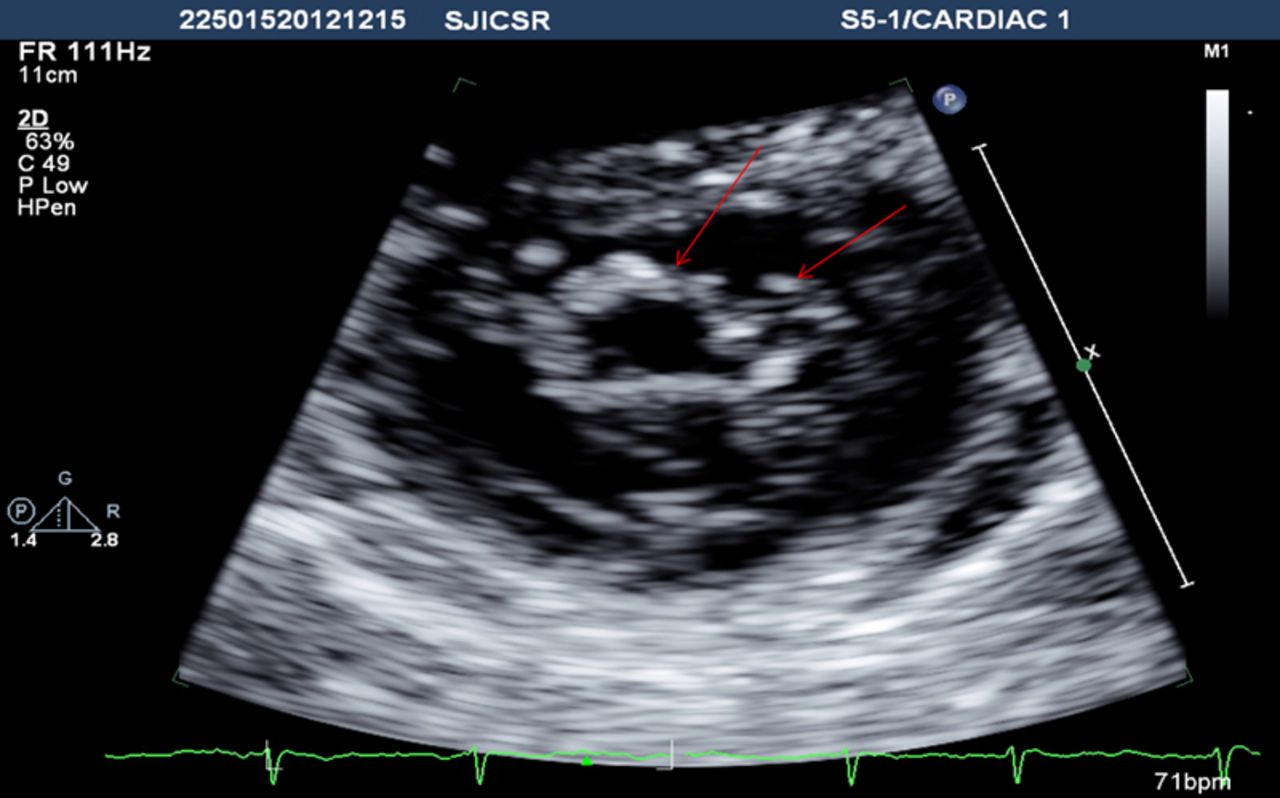
Modified short axis view showing two mitral orifices.

Modified short axis view showing two mitral orifices (in different angulation).

Modified short axis view showing mitral valve area.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Apical four-chamber view with calculation of gradient across mitral valve.
Parasternal long axis view showing subvalvular disease.
Parasternal short axis view showing valvular & subvalvular orifice.
Parasternal short axis view with colour Doppler showing 2 jets of forward flow through mitral valve(1 from valvular orifice and other from subvalvular orifice).
Apical 4 chamber view showing subvalvular orifice.
The valve described here, resembled double-orifice mitral valve (DOMV). Differentiating features were history of rheumatic fever in childhood, thickened valve leaflets, severe subvalvular disease with existence of two papillary muscles.
Most common cause of mitral stenosis is rheumatic heart disease.1 Twenty five percentage of rheumatic heart disease patients have isolated mitral stenosis, 40% have combined stenosis and regurgitation.1 ,2 About 70% of all patients with rheumatic mitral stenosis are women. Diagnostic findings on echocardiography are leaflet thickening, chordal shortening with fusion. DOMV may be stenotic, regurgitant or normal.3 Commonly associated anomalies with DOMV are atrioventricular, ventricular or atrial septal defects, Ebstein anomaly, tetralogy of Fallot, coarctation of aorta.
Learning points
-
Rheumatic mitral stenosis can simulate double-orifice mitral valve in presence of severe subvalvular fusion.
-
Meticulous echocardiographic examination can differentiate between two entities by taking different views and also reduce the financial burden for the patient for costlier investigations like 3 dimensional echocardiogram.
-
Parasternal short axis view taken alone can be quite confusing.
Footnotes
-
Contributors All authors were involved in the patient care and the manuscript writing.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.