Article Text

Statistics from Altmetric.com
Description
A 21-year-old man was admitted to the urology department due to swelling and pain in the left inguinal region. On initial physical examination, he was slightly febrile, and areas of induration with tenderness were palpated in the left inguinal region and left hemiscrotum. Laboratory tests showed leukocytosis (14 000/mm3) and elevated C reactive protein (12 mg/dL). On ultrasound left epididymo-orchitis and expansion of the left inguinal canal were seen. In addition, a cystic tubular mass with wall thickness that had displaced the bladder was seen in the left hemipelvis (figure 1). Contrast-enhanced CT revealed a cystic tubular mass with marked marginal enhancement from the left inguinal canal to the left seminal vesicle. On MRI the finding of left epididimo-orsitis and expansion of the left spermatic cord with tubular fluid collection was determined. On contrast-enhanced MRI the left spermatic cord abscess was confirmed. Abscess formation of the prostate tissue was not observed. Moreover, the mild wall enhancement of the seminal vesicle and mild cystic dilation were seen. Surgical intervention was not considered in the first place due to the reduction in the patient’'s complaints after treatment with antibiotics and localised spermatic cord abscess. He was discharged 15 days after being admitted to the hospital (figures 2⇓–4).

Ultrasound images show expansion of the left inguinal canal (A) and a cystic tubular mass with wall thickness that had displaced bladder in the left hemipelvis (B).

Contrast-enhanced CT image shows a cystic tubular mass with marked marginal enhancement from the left inguinal canal to the left seminal vesicle.

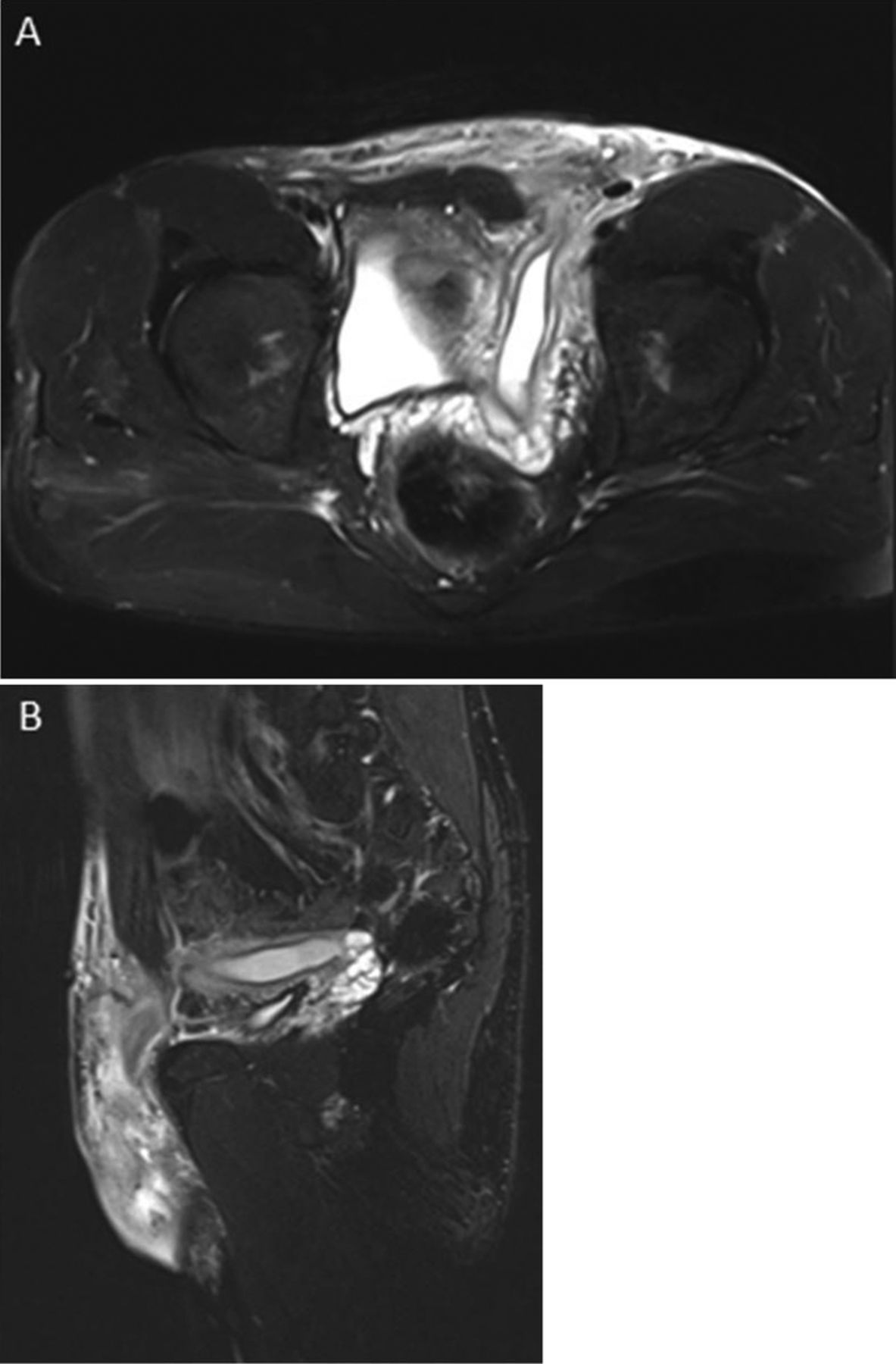
Axial (A) and sagittal (B) T2-weighted MRI show the finding of left epididimo-orsitis, expansion of the left spermatic cord with tubular fluid collection and subcutaneous oedema of the left inguinal area.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Axial (A) and sagittal (B) contrast-enhanced MRI show left spermatic cord abscess.
Spermatic cord abscess is generally secondary to inflammation of the prostate. The suggested pathological mechanism is that a retrograde urinary infection moves through the ductus deferens to the spermatic cord.1 In the literature spermatic cord abscesses due to Escherichia coli and Candida have been determined in two different cases.1 ,2 To our knowledge, ours is the third report in the literature. However, ours is the first case that did not have chronic diseases.
Learning point
-
On imaging modalities, spermatic cord abscess should be considered when cystic tubuler mass is seen in hemipelvis.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.