Article Text

Statistics from Altmetric.com
Description
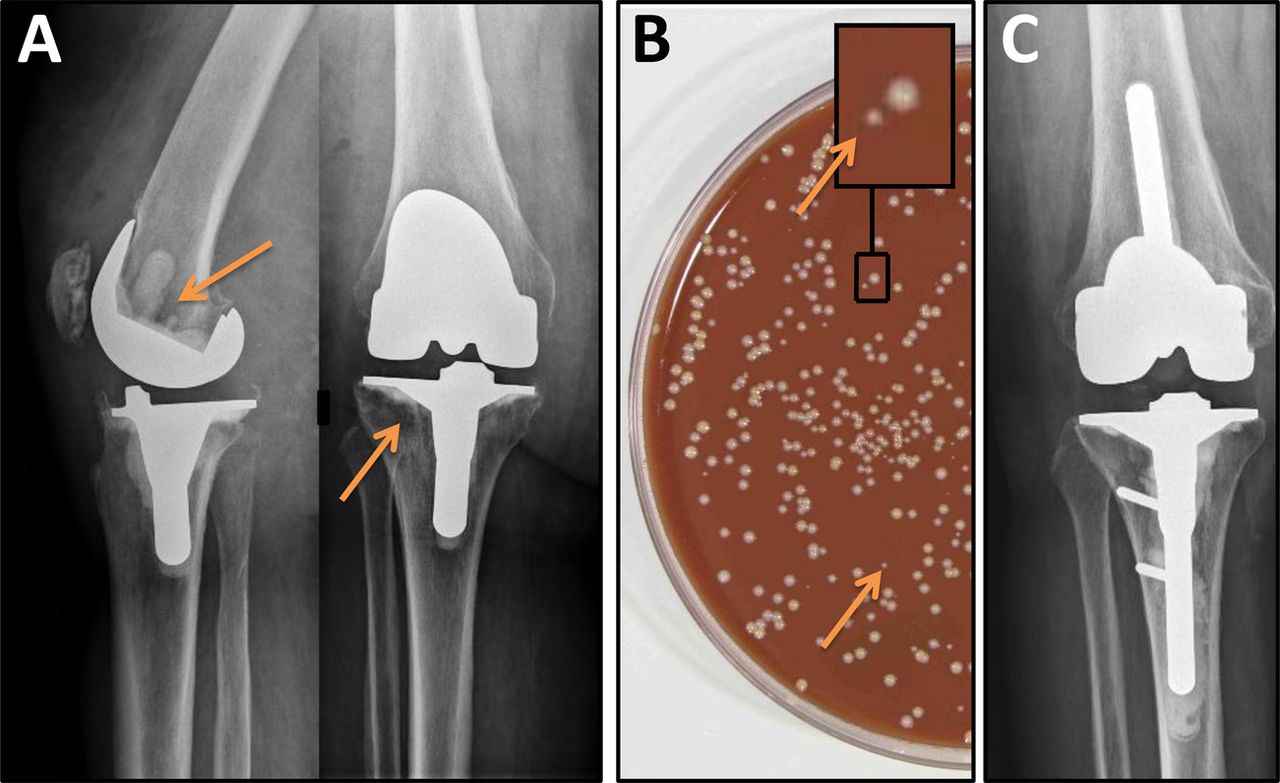
An 80-year-old woman with a history of β-lactam allergy was admitted for chronic knee prosthesis joint infection (PJI) (figure 1A). The prosthesis was removed and sonicated as previously described (400 ml of Ringer solution was added in a sterile box containing the explanted prosthesis, vortexing was performed before and after sonication in ultrasound bath, and then 100 μl of sonicate fluid was plated onto aerobic and anaerobic medium and broth).1 All peroperative samples revealed methicillin-susceptible Staphylococcus aureus in cultures, whereas the sonicate fluid culture yielded additional S aureus small colony variant phenotype (SCV) (figure 1B). Vancomycin (1 g/day intravenously) followed by rifampin (1200 mg/day orally) were started. As a rash with eosinophilia occurred, vancomycin and rifampin were switched to daptomycin 850 mg/day (9 mg/kg/day). Reimplantation, performed after a 6-week interval, did not reveal any bacterial growth in culture. Daptomycin was continued for a total duration of 3 months, with perfect clinical and biological tolerance. At 1-year follow-up, clinical and radiological outcomes were favourable (figure 1C).
{kind=link}
Periprosthetic pathological lucencies (A, arrows), associated with MSSA SCV in cultures (small colonies) obtained with sonication from prosthesis explantation (B, arrows). After reimplantation and a total of 3 months of antimicrobial therapy, no relapse occurred at 1 year (C, x-ray).
S aureus, one of the most frequent aetiological agent of PJI, is associated with a high rate of relapse, partly explained by its capacity to produce biofilm and to convert into SCV, which is a slow-growing phenotype associated with intracellular persistence.2 Our case highlights that (1) sonication should help to isolate these phenotypic variants, actually underestimated due to fastidious growth requirements; (2) prolonged high dose (≥8 mg/kg/J) of daptomycin (considered as an alternative for the treatment of S aureus PJI at the standard dose of 6 mg/kg/J3) might be efficient in patients with chronic PJI due to SCV expressing S aureus. In fact, as it was demonstrated for rifampin (compromised in our case), recent studies pinpointed the antibiofilm activity of daptomycin. Its antimicrobial activity against SCV remained to be investigated.
Learning points
-
Sonication may help to show small colony variant phenotype in Staphylococcus aureus chronic prosthesis joint infection.
-
Daptomycin could be used for the treatment of S aureus chronic prosthesis joint infection.
Acknowledgments
We acknowledge Dr Franck Trouillet who participated to the patient care and all our colleagues from the Lyon Bone and Joint Infection study Group: Physicians—Tristan Ferry, Thomas Perpoint, André Boibieux, François Biron, Florence Ader, Anissa Bouaziz, Judith Karsenty, Fatiha Daoud, Johanna Lippman, Evelyne Braun, Marie-Paule Vallat, Patrick Miailhes, Florent Valour, Christian Chidiac, Dominique Peyramond; Surgeons—Sébastien Lustig, Franck Trouillet, Philippe Neyret, Olivier Guyen, Gualter Vaz, Christophe Lienhart, Michel-Henry Fessy, Cédric Barrey; Microbiologists—Frederic Laurent, François Vandenesch, Jean-Philippe Rasigade; Nuclear Medicine—Isabelle Morelec, Emmanuel Deshayes, Marc Janier, Francesco Giammarile; PK/PD specialists—Michel Tod, Marie-Claude Gagnieu, Sylvain Goutelle; Clinical Research Assistant—Marion Martinez.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.