Article Text

Summary
This is a case of a patient who presented with generalised weakness, dysphagia and ptosis. Upon evaluating the patient, she was found to have myasthenia gravis (MG) with anaemia and hypothyroidism. Further evaluation for the cause of anaemia revealed that the patient had pure red cell aplasia (PRCA). CT thorax revealed a thymoma. The patient was given packed cell transfusions, steroids and pyridostigmine. The patient improved symptomatically. Her haemoglobin level at follow-up was 9.5 gm/dl. The patient has been posted for thymectomy. This is a rare case of PRCA seen in a patient with MG, with thymoma associated with hypothyroidism.
Statistics from Altmetric.com
Background
Myasthenia gravis (MG) is characterised by antibodies to acetylcholine receptors at the neuromuscular junction. Thymic abnormality in the form of thymic hyperplasia (65%) or thymoma (10%) is the most common of the associations of MG.1 MG and thymoma are associated with a variety of autoimmune conditions, including autoimmune thyroiditis, Grave's disease, rheumatoid arthritis, systemic lupus erythematosus, type 1 diabetes mellitus, etc.2 This is a report of an uncommon association between MG and pure red cell aplasia (PRCA). Anaemia in a patient of MG can occur owing to pernicious anaemia, PRCA and auto immune haemolytic anaemia. MG appears in about 20–40% of patients with thymoma and PRCA develops in about 2–5% of those patients. On the other hand, thymoma is detected in 10% of patients with MG and in 5–13% of patients with PRCA.3 Anaemia in MG should be thoroughly evaluated to find its cause. Knowledge of the causes of anaemia in case of MG is important to work up the patient and manage the patient as most of these cases are curable.
Case presentation
A 55-year-old lady, symptomatic since 1.5 month, came to us with a history of drooping of both the eyelids, dysphagia and limb weakness with symptoms worsening as evening approached. History of generalised weakness with easy fatiguability was present. There was no history of recent weight loss or loss of appetite, blood loss from any site, or drug intake. Upon examination, the patient had marked pallor. There was no icterus or lymphadenopathy. Bilateral fatiguable ptosis was present. Gag reflex was preserved. Limb power was grade 3/5. Reflexes were 2+ and there was no muscle wasting.
Investigations
Upon investigation, the patient's haemoglobin was found to be 4.8 g%. Her red blood cell count was 1.1×106/mm3, with a reticulocyte count of 0.5%. Total white blood cell count was 5600/mm3 and platelet count was 0.2×106/mm3. Her acetyl choline receptor antibodies was strongly positive 14.7 (>0.4 being positive). Direct and indirect Coomb's test were negative. Patient's antinuclear antibody and dsDNA (double-stranded DNA) were negative. Repetitive nerve stimulation test was done which showed a decremental response in orbicularis oculi and nasalis muscles suggestive of postsynaptic neurotransmission defect, conclusive of MG. Chest x-ray showed a mediastinal mass with positive silhouette sign (figure 1). Chest CT showed a well-defined, homogeneous, minimally enhancing mass lesion 7.1×9.5 cm in the anterior mediastinum suggestive of thymoma. Fat planes around the mass were maintained. Evidence of calcification within mass was present. Lung window was normal (figure 2). barium swallow was also normal.

Chest x-ray showing a mediastinal mass with positive silhouette sign.
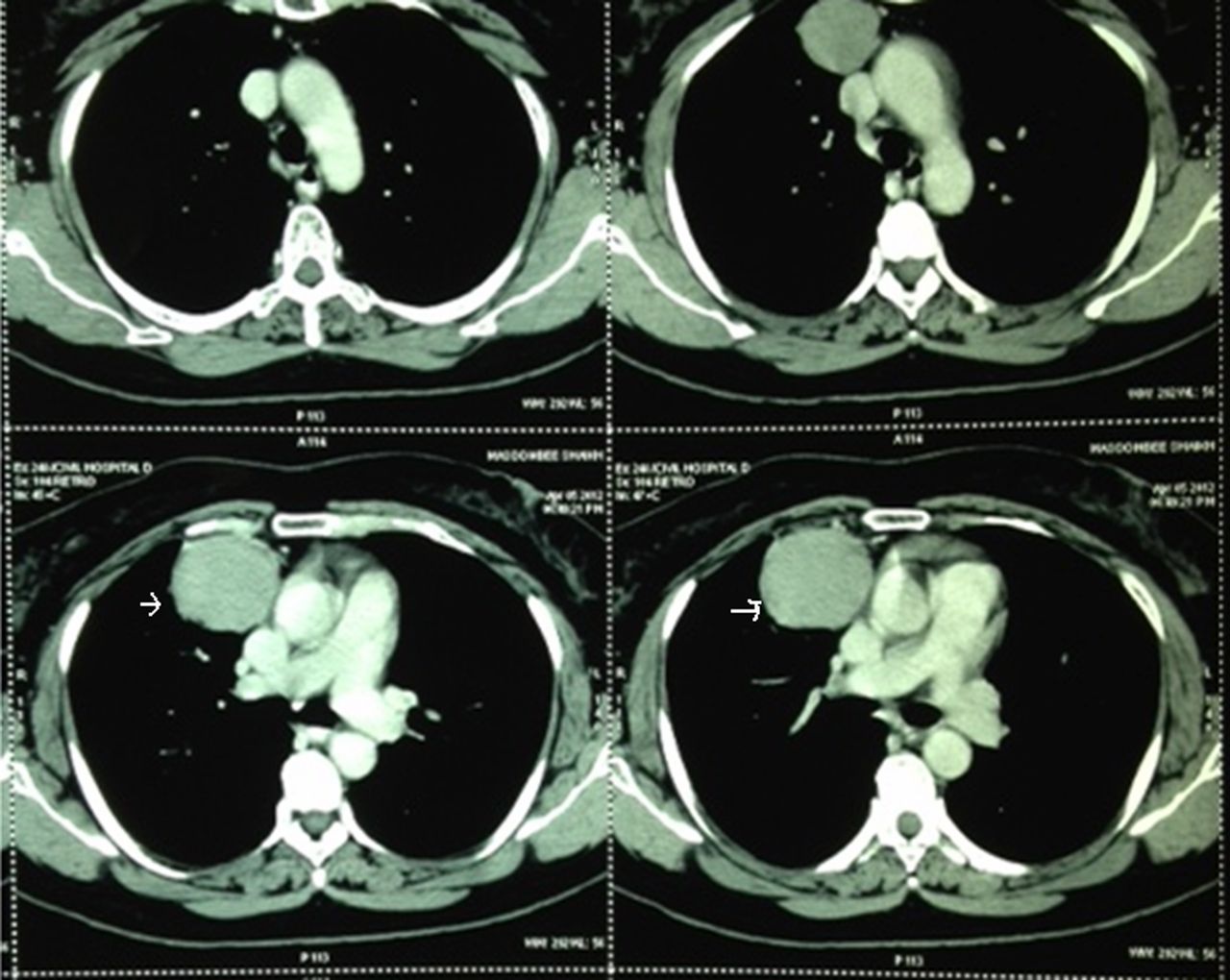
Chest CT showing a well-defined, homogenous, minimally enhancing mass lesion 7.1×9.5 cm in the anterior mediastinum suggestive of thymoma.
Thyroid function tests showed T3 of 53.6 ng/dl (77–135 ng/dl) and T4 of 4 µg/dl (5.4–11.7 µg/dl), both suppressed; thyroid stimulating hormone (TSH) was elevated to 11.8 µIU/ml (0.34–4.25 µIU/ml); antimicrosomal antibody was positive 108.50 U/ml with more than 40 being significant. These reports were suggestive of autoimmune hypothyroidism.
B12 levels were 378 pg/ml (279–996 pg/ml). Serum iron studies revealed iron of 78 µg/dl (normal 40–180 µg/dl), and iron binding capacity of 288 µg/dl (normal range 250–440 µg/dl).
Bone marrow aspiration was done. Bone marrow revealed a normocellular aspirate with markedly reduced erythroid precursors. No mature normoblasts were seen. Occasional proerythroblasts were seen. Myeloid series showed relative hyperplasia with all stages of maturation. Megakaryocytes were normal. Bone marrow examination was suggestive of PRCA (figure 3).

{kind=link}
{kind=link}
{kind=link}
Bone marrow aspiration showing a normocellular aspirate with markedly reduced erythroid precursors. No mature normoblasts were seen. Occasional proerythroblasts were seen. Myeloid series and megakaryocytes were normal.
A final diagnosis of MG with thymoma with PRCA with autoimmune hypothyroidism was made.
Treatment
The patient was given packed cell transfusions for correction of anaemia; prednisolone 50 mg once daily for 1 month followed by tapering by 5 mg every 2 weeks was started. Pyridostigmine was started at a dose of 60 mg four times a day. The patient was also started on thyroxine 50 μg daily for her hypothyroidism.
Outcome and follow-up
Three weeks after admission, during routine follow-up, the patient reported an improvement in her muscle strength and general well-being. Currently, the patient does not have ptosis or dysphagia and her power is grade 5/5 in all four limbs. Her haemoglobin at the last follow-up was 9.5 g%. The patient required no further transfusions and is doing well. The patient is awaiting thymectomy.
Discussion
MG is an autoimmune disorder characterised clinically by weakness and easy fatigability of skeletal muscles, which improves with rest. Immunopathogenesis of this disorder involves a reduction in the number of junctional nicotinic acetylcholine receptors (AChRs) present on skeletal muscles, brought about by an antibody-mediated attack against the AChRs.
The simultaneous occurrence of MG, PRCA and thymoma is extremely rare. MG appears in about 20–40% of patients with thymoma, and PRCA develops in about 2–5% of those patients. On the other hand, thymoma is detected in 10% of patients with MG and in 5–13% of patients with PRCA.4 About 50% of the patients with PRCA suffer from thymoma. Conversely, because PRCA is rare, it occurs in only 5% of patients with thymoma. Our patient in addition also had autoimmune thyroiditis with hypothyroidism. To the best of our knowledge, the association of MG, PRCA, thymoma and autoimmune thyroiditis has not been reported.
Anaemia in a case of MG can be nutritional anaemia, autoimmune haemolytic anaemia, pernicious anaemia or PRCA. The latter is highly uncommon. The patient should undergo a detailed evaluation, including, serum iron studies, serum B12 levels, direct and indirect Coomb's test, anti-intrinsic factor and antiparietal cell antibodies and a bone marrow examination. Pernicious anaemia owing to antibodies against gastric parietal cells and/or intrinsic factor has been reported.5 The same can be confirmed by the measurement of the antibodies using immunoflorescence technique. The association between MG and pernicious anaemia is believed to be a common autoimmune process. Autoimmune haemolytic anaemia owing to antibodies against red blood cells is also known to occur in MG. In this case the Coomb's test would be positive.3
PRCA is characterised by normocytic anaemia, reticulocytopenia and severe erythroid hypoplasia of the bone marrow associated with normal myeloid and megakaryocytic cell lines. It is divided into congenital and acquired categories, the latter being further subdivided into two subclasses—primary and secondary.6 Four different immune pathogenetic mechanisms of development of PRCA in MG have been demonstrated. These include antibodies to erythroblasts, to erythropoietin-responsive cells and to erythropoietin, in addition to T-cell suppression of erythropoiesis. A thymoma or the thymus might have an antigen in common with the erythroblastic cells. On the other hand, thymectomy results in remission in 30% of cases.7 Although thymic excision in the absence of a thymic mass has been advocated by some, it remains of unproven value. Other treatment options include steroids and immune suppressive drugs like cyclophosphamide and azathioprine. In treatment-resistant patients, antithymocyte globulin may be effective. Some patients post-thymectomy may need continued immune suppression to maintain remission.
Chest x-ray and CT scan are indicated in patients with autoimmune thyroiditis to search for a thymic mass. Conversely, a search for autoimmune thyroiditis is warranted in patients with an identified thymic mass. In a study by Wolfgang et al, evaluation of thyroid function in 104 patients with MG by T3, T4, TBG and TSH radioimmunoassays, disclosed thyrotoxicosis in 5.7%, preclinical hyperthyroidism probably owing to autonomously functioning thyroid tissue in about 10% of patients stimulated with TRH, hypothyroidism in 1.9% and preclinical hypothyroidism in 3.4%. Eighty-four percent were euthyroid. Twelve patients had antithyroglobulin antibodies (Tab), and 28 had antimicrosomal antibodies (Mab). Among the euthyroid MG patients, 7 were Tab-positive and 20 were Mab-positive. Euthyroid antibody-positive patients had a significantly higher risk for hypothyroidism.8 Hypothyroidism should be suspected, especially if a patient with MG has persistent symptoms even upon treatment.
Knowledge of these associations of MG with other autoimmune conditions and of the potentially treatable causes of anaemia is important so as to diagnose them early and manage them appropriately. Till date very few cases of MG with thymoma and PRCA have been published. But to the best of our knowledge there is no case published with the above three with hypothyroidism.
Learning points
-
A patient of myasthenia gravis (MG) should be investigated for association of other autoimmune conditions.
-
Pure red cell aplasia (PRCA) as a rare cause of anaemia in patients with MG should be thought of and investigated accordingly.
-
Thymectomy may be curative for MG and PRCA in patients with thymoma or thymic hyperplasia.
-
Autoimmune hypothyroidism is a rare association of MG with thymoma and should be looked for in all patients especially those who have persistent symptoms on treatment.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.