Article Text

Statistics from Altmetric.com
Description
A patient diagnosed with an International Federation of Gynaecology and Obstetrics Stage-IB2 cervical carcinoma was referred to us for radiation-based treatment, given the evidence for equivalence of surgical and radiotherapeutic managements.1 In preparation for standard chemoradiotherapy (a plan of three-dimensional conformal radiotherapy with concurrent cisplatin chemotherapy followed by brachytherapy), the patient underwent a CT scan as part of the RT planning process. Surprisingly, the presence of an ectopic pelvic kidney was noted (figure 1). Noting the normal excretion of contrast in the ipsilateral ureter, the pelvic kidney was functional in all probability (figure 2).

Volumetric reconstruction of the pelvic CT scan demonstrating the ectopic location of the right kidney (maroon). Also seen are the left-kidney (dark blue) and the urinary bladder (cyan).

Axial CT slice demonstrating the location of the right-kidney within the pelvic cavity. The functionally intact kidney is shown to excrete contrast into the ipsilateral ureter (white arrow).
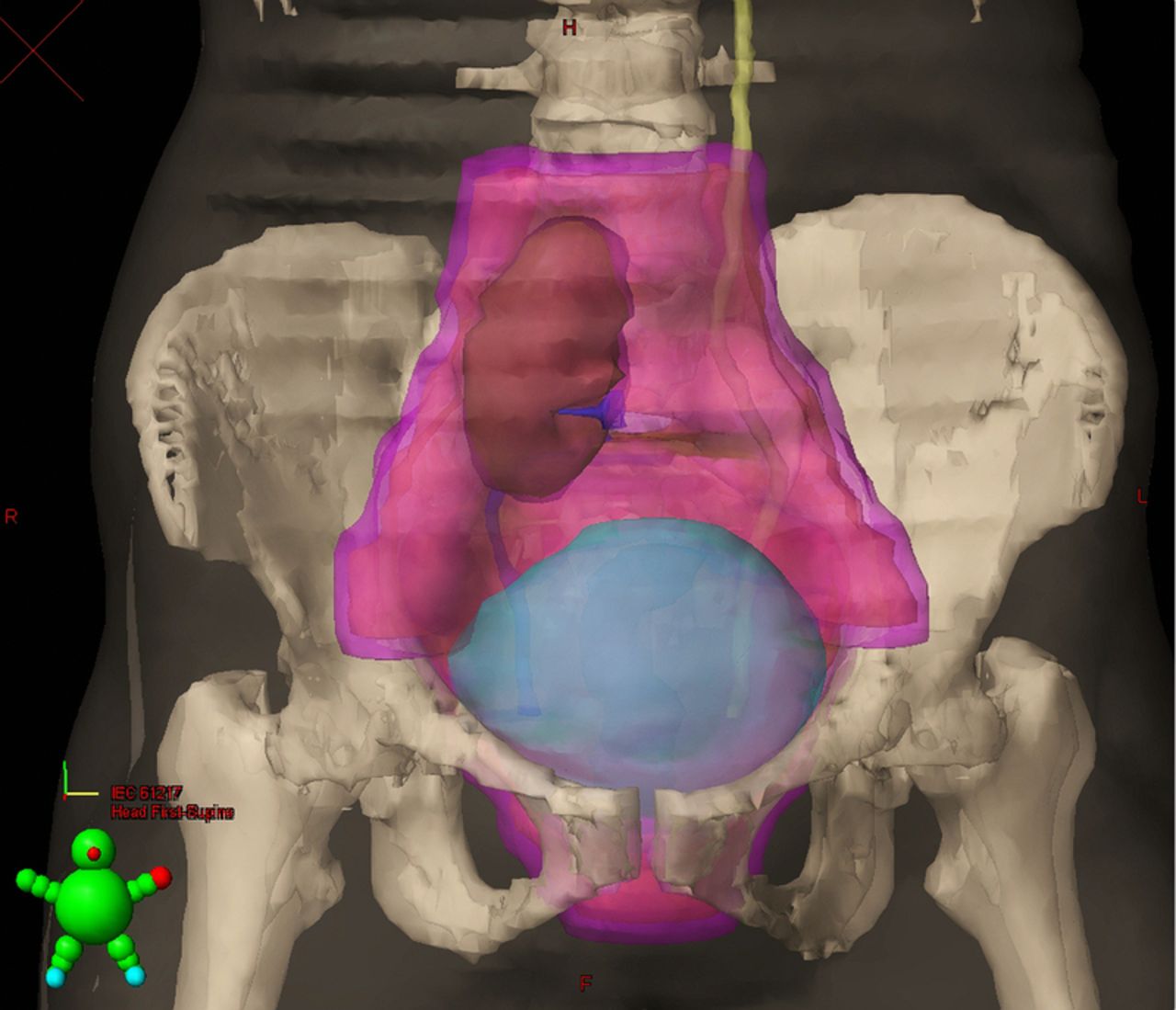
Given the early stage (IB2), we had the luxury to cancel RT and to opt for radical hysterectomy. The standard RT portals for cervical carcinoma targets the disease, as well as the pelvic-lymphatics including the common, internal and external iliac lymph nodes, along with the obturator and presacral lymph nodes (figure 3). Thus, the use of pelvic external-beam RT (to a dose of 45–50 Gy) would have easily exceeded the tolerance limits of the pelvic kidney (estimated as 28 Gy for a 50% risk of complications at 5 years).2

{kind=link}
{kind=link}
{kind=link}
The right kidney is shown in relation to the clinical target volume (pink shaded volume) which includes the primary disease and the pelvic lymph nodes.
The pelvic kidney results from the failure in normal ascent of a kidney, and is known to have an incidence of one in 2000–3000 persons. The affected patients are usually asymptomatic, with the involved kidney being functionally normal.3
In the possible scenario wherein a patient with a pelvic kidney presents with a cervical cancer staged beyond IIA, the use of RT becomes mandatory. In such situations, the use of intensity-modulated radiotherapy would be able to deliver adequate doses of radiation to the primary disease and the nodal areas, while at the same time sparing the pelvic kidney from overdose.4
Learning points
-
The non-use of sectional imaging prior to the initiation of radiotherapy may render the clinician oblivious to the presence of a pelvic kidney.
-
The treatment of early-stage carcinoma of the cervix in the presence of a pelvic kidney is better attempted with surgery than with radiotherapy.
-
For locally advanced carcinoma of the cervix, where the use of radiotherapy is warranted, it is better attempted with intensity-modulated radiotherapy, which holds the potential to spare the pelvic kidney while at the same time delivering desired doses of radiation to the target primary and nodal areas.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.