Article Text

Statistics from Altmetric.com
Description
A 62-year-old woman presented with a 2-year history of abdominal pain, weight loss and diarrhoea. Her medical history included well-controlled epilepsy, migraine, hypothyroidism and depression with previous drug overdose. She was a long-term smoker. She had been referred to gastroenterology outpatients twice already by her general practitioner as suspected malignancy.
She described a 2-year history of worsening epigastric and more generalised abdominal pain that was typically postprandial and dull and ‘gnawing’ in nature. Pain was usually followed by non-bloody diarrhoea occurring up to seven times a day. She reported that pain was limiting her oral intake and over the last few months she had lost approximately one stone in weight. Of note, her husband had died 2 years previously.
Physical examination was unremarkable except for her marked slimness. Her body mass index (BMI) in clinic was 14.7 (16.0 6 months previously).
Negative investigations to date included: grossly normal bloods (with the exception of an elevated thyroid-stimulating hormone), normal flexible sigmoidoscopy and CT abdomen/pelvis with contrast. Upper gastrointestinal endoscopy revealed mild gastritis with gastric biopsies demonstrating helicobacter but normal duodenal histology. Uncomplicated gallstones were noted on abdominal ultrasound.
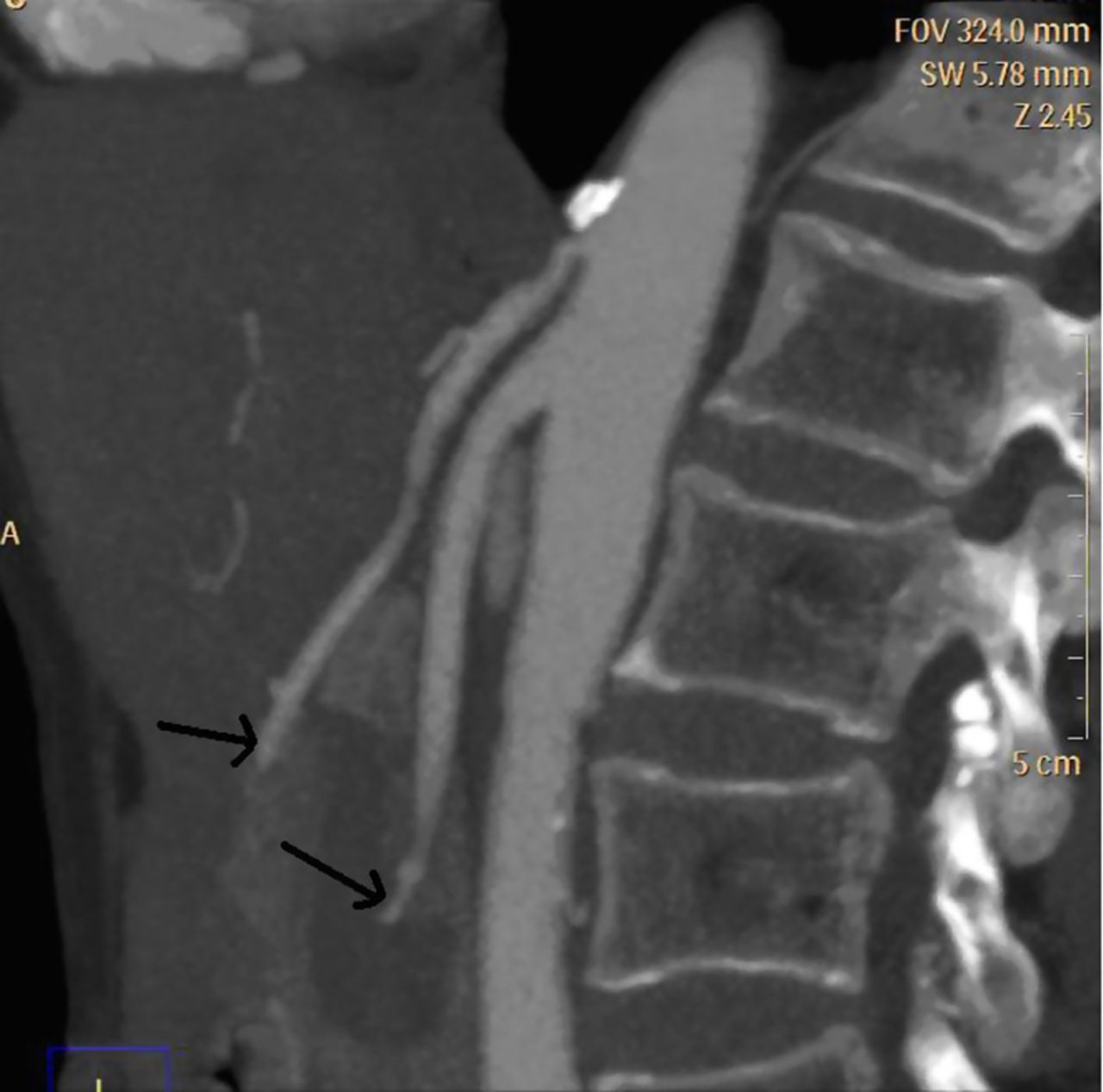
She subsequently underwent a CT mesenteric angiogram and this demonstrated stenosis of the coeliac and superior mesenteric arteries (figure 1) and she was given the diagnosis of chronic mesenteric ischaemia (CMI).

{kind=link}
CT mesenteric angiogram demonstrating stenosis of the coeliac and superior mesenteric arteries.
Mesenteric ischaemia may be chronic or acute, single or multivessel. Traditionally, diagnosis was thought to require a significant stenosis of at least two of coeliac, superior mesenteric and inferior mesenteric arteries; however, it has subsequently been demonstrated that single arterial stenosis is sufficient to induce the syndrome.1 Atherosclerosis and occasionally vasculitic processes may cause CMI. Atherosclerotic gastrointestinal and cardiovascular risk factors are identical and atherosclerosis was identified in our patient, a life-long smoker.
CT or MR angiogram are investigations of choice; traditional angiograms are invasive and do not provide information about surrounding structures.
Treatment is directed at symptoms, nutrition and prevention of bowel infarction. Conservative treatment comprises antiplatelet therapy with nutritional support and ‘watch and wait’. For occlusive disease or where risk of infarction is imminent, intervention is required. Approach may be percutaneous, laparoscopic or open vascular surgery.1 Our patient declined endovascularisation and was instead started on low-dose aspirin and nutritional supplements. Six months on she was pain free and her BMI had increased to 16.8.
Learning points
-
A low threshold of suspicion for chronic mesenteric ischaemia is necessary when faced with marked unexplained weight loss and abdominal pains. Our patient was diagnosed on CT angiogram, but not before she had been misdiagnosed as depressed with a potential eating disorder.
-
Occlusion or disease of one of the coeliac, superior mesenteric or inferior mesenteric arteries is sufficient to cause symptoms and may be bowel threatening.
-
Treatment is directed at symptoms, nutritional state and prevention of bowel infarction.
Reference
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.